


Carrying in Special Circumstances
Sometimes there is a need for extra support with using slings; don’t be discouraged if you or your child have extra needs, there are always ways to keep carrying in special circumstances.
If your child can be held and carried in arms, there is likely to be a way to carry them safely in a sling. Twins can be carried in slings, as can a baby and a toddler at the same time (tandem carrying). There are ways to carry safely in pregnancy, to carry after birth, to carry premature babies. We will help you to carry your child if you have a disability, or if your child has special needs or physical health concerns. We are here to help you find a way to keep them close.
This page links to some useful information; personal stories about carrying in special circumstances, professional advice and useful links. Please see our Common Queries page for simpler situations.
If you have a special story, please get in touch to share them with me for the wider community!
I also recommend the Tania Talks blog posts on babywearing (she is a wheelchair user)
https://www.whentaniatalks.com/the-realities-of-back-carrying-as-a-wheelchair-user/
https://www.whentaniatalks.com/back-carrying-as-a-wheelchair-user/
















Here is an excellent downloadable article on Potential Therapeutic Benefits of Babywearing by Robyn Reynolds-Miller.
You can find more educational resources here for downloading (such as infographics and leaflets and images)
If you need more specialised support or have a query not covered here, please do get in touch with me or find your local sling library at Sling Pages.

Carrying a Premature Baby, personal story
This is Kay and Alex's story of carrying a premature baby. She tells us about their lives together and what role slings have played in their rocky journey. It is a truly inspiring story of great courage and endurance and I am honoured to have played a small part.
"For as long as I can remember I have wanted to be a mum, but my real journey to parenthood started 5 years ago. I decided that I didn't want to wait for the "right person" to come along and started looking into fertility treatment for single women. Unfortunately the process wasn't was easy as I expected; after lots of tests and surgery I discovered that I had endometriosis which may affect fertility..
I started out doing IVI with donor sperm but after two attempts with no success it was suggested that IVF might have a better chance of working. I decided to take part in the egg-sharing programme to reduce the cost and hopefully help someone else too. During this time there was a lot of compulsory counselling to ensure I was aware of all potential outcomes. I'm very lucky that I have a fantastic support system of family and friends around me, especially my parents.
The first attempt at IVF was not straightforwards, I got 14 eggs, (7 of which were donated), but only one was fertilised. This was put back and I got a chemical pregnancy but miscarried. I also got a relatively rare condition called Ovarian Hyperstimulation Syndrome (OHSS) which made me really ill and I had to be hospitalised on numerous occasions. Due to the poor fertilisation rate it was thought that I had poor egg quality so had to pay the full cost of IVF treatment (as a single woman I was not entitled to any NHS treatment.)
On the second IVF attempt, medications were reduced to try lessening the risk of OHSS but because doctors were anxious about this, the egg collection was done too early and 5 eggs were lost during retrieval. This attempt was unsuccessful. I again got OHSS but much milder this time. The emotional rollercoaster or IVF is unimaginable and the hormones of treatment don't help! You spend all your time so focused on preparing to become pregnant, trying to stay positive, eat well etc, then once the embryo is implanted you have the longest two weeks praying you are pregnant and counting down to the day you can take a pregnancy test... but as soon as it is test day comes you don't want to do the test because you are until then "Pregnant till Proven Otherwise" ( PUPO). Internet support groups become your sanctuary because others undergoing IVF can understand what you are feeling, while your family and friends sometimes don't understand why you put yourself through so much. IVF became my only focus.
After the second attempt I had an eight month break to save up as I had used all my savings. I decided that the next would be my last attempt and I would do everything I could to try to help it work so I would have no regrets. I changed my diet (cutting out all processed food), saw a nutritionist, had regular massage (including Mayan abdominal massage) and acupuncture. We changed the IVF regime to one that had a higher chance of success but also a higher risk of OHSS. It was a risk I was willing to take. I had partly given up hope of this round working, as I got two fertilised eggs out of 19 when I began getting the OHSS symptoms again on day 2.
I did a home pregnancy test two days before test day..... and it was positive!
I didn't know how to react, so burst into tears before laughing maniacally then calling my best friend and my parents. The excitement wore off quickly though when I was admitted to hospital with OHSS at just 4+1 weeks. At a point when I had hoped that the hard part was over, it turned out that this was just the beginning of another difficult journey.
 At 18 weeks pregnant, I began getting tightenings. As a midwife, I knew that Braxton Hicks could start early, so I just assumed it was this. though I also worried it might be something more. At 19+4 with continued tightenings, I was seen by my consultant for review and thankfully everything looked ok and possibly just a urine infection causing all this. I was reassured two days later when I had my anatomical scan and everything looked good with a healthy active baby.
At 18 weeks pregnant, I began getting tightenings. As a midwife, I knew that Braxton Hicks could start early, so I just assumed it was this. though I also worried it might be something more. At 19+4 with continued tightenings, I was seen by my consultant for review and thankfully everything looked ok and possibly just a urine infection causing all this. I was reassured two days later when I had my anatomical scan and everything looked good with a healthy active baby.
I continued to have tightenings but tried to ignore them as everything else seemed OK. Then exactly two weeks later after my scan at 21+6, I started with the smallest amount of bleeding. Again I was reassured as baby seemed OK and it had settled, possibly caused by a cervical erosion, and just to observe. I continued spotting on and off but nothing major, until I was at work on a shift on labour ward at 23+1 weeks pregnant.
I had a significant bleed and was terrified. I felt it was too far on in the pregnancy to lose the baby now but it was far too early to be born. I burst into tears. I am so grateful that I was at work surrounded by fantastic colleagues. I was admitted to the antenatal ward for observation overnight and I didn't go home again.
I continued to have tightenings and bleeding to varying degrees over the next three weeks. Getting to 24 weeks was a major milestone and I was given steroids to mature the baby's lungs. At around 25 weeks my waters went though because of the bleeding it wasn't obvious. Baby was breech and because of the situation I kept being told I might be taken for a Caesarean if bleeding increased or I went into labour. I saw paediatricians who told me stark statistics about survival rates and disability. As a midwife I knew these things but as a mum it just didn't sink in. I was tearful and losing hope. At 25+5 I had a major bleed that got me taken to labour ward and starved in case it continued and and I needed theatre. I spent the next two days in high dependency being observed and in denial.
Writing it down now it seems so silly but even given the bleeding, tightenings and water break it still never clicked to anyone that the pain I was in could be labour. At exactly 26 weeks I was found to be 7cm dilated. Two hours later I had a vaginal breech delivery complicated by the head getting stuck.
Alexander Benjamin was born weighing 1lb 12 oz and in a very poor condition.

The room was full of people but no-one was saying a word. Looking back at his notes now it says it took 18minutes to stabilise him before taking him to intensive care but it didn't feel that long to me. It seems awful to think about it now but at that point once Alex was born all I felt was relief. I was glad the pregnancy was finally over after months of feeling ill and stressed. I had spent the last few weeks trying to detach from the pregnancy as I feared the worst, but in the moment when Alex was taken away and we (myself, my parents and my friend) were left alone the silence said it all.
 I know it can often take up to an hour to get a baby settled into neonatal unit with all the lines, Xrays etc so we patiently waited. After nearly two hours I went to ask if we could see him.. the midwife came back saying the consultant wanted to come and talk to us first. I know the language of medical professionals and I honestly thought we had lost him. The consultant came round and told us that "Alex is a very sick little boy" and that the first 24hours would be critical. I think the adrenaline stopped me from feeling the full effects of the situation but looking back now at pictures and videos of those first hours has me choked up. Alex was beautiful to me, but so frail. You can count every rib and due to the manipulation of delivery his leg is almost black with bruising. He was covered with monitoring leads and various IV lines plus on a ventilator to keep him alive. He was put under phototherapy immediately.
I know it can often take up to an hour to get a baby settled into neonatal unit with all the lines, Xrays etc so we patiently waited. After nearly two hours I went to ask if we could see him.. the midwife came back saying the consultant wanted to come and talk to us first. I know the language of medical professionals and I honestly thought we had lost him. The consultant came round and told us that "Alex is a very sick little boy" and that the first 24hours would be critical. I think the adrenaline stopped me from feeling the full effects of the situation but looking back now at pictures and videos of those first hours has me choked up. Alex was beautiful to me, but so frail. You can count every rib and due to the manipulation of delivery his leg is almost black with bruising. He was covered with monitoring leads and various IV lines plus on a ventilator to keep him alive. He was put under phototherapy immediately.
Only I was allowed to touch him but couldn't hold him yet.
 My first hold came on November 17th, aptly, World Prematurity Day. I was nervous about pulling a line or hurting him but also so excited to hold him! He was put skin to skin down my top and his ventilator tubes taped to me to keep him safe. I can still smell him now and it brings me to tears. As a parent you take for granted the milestones you will see; the birth experience you imagined, the crying baby just born and put skin to skin at once. I didn't get these, and my milestones with Alex are different, but even more amazing after the challenges he has faced. We spent 135 days in the neonatal unit and I was there 12 hours a day for 133 of those days. (Two days I was ill from sheer exhaustion and wasn't allowed in.)
My first hold came on November 17th, aptly, World Prematurity Day. I was nervous about pulling a line or hurting him but also so excited to hold him! He was put skin to skin down my top and his ventilator tubes taped to me to keep him safe. I can still smell him now and it brings me to tears. As a parent you take for granted the milestones you will see; the birth experience you imagined, the crying baby just born and put skin to skin at once. I didn't get these, and my milestones with Alex are different, but even more amazing after the challenges he has faced. We spent 135 days in the neonatal unit and I was there 12 hours a day for 133 of those days. (Two days I was ill from sheer exhaustion and wasn't allowed in.)
 I spent my time holding Alex as much as I could and when he was too poorly to be held I touched him through the incubator and spoke and sang to him. I felt being physically close would help us both bond better, especially after an awful pregnancy and so much separation. I was already aware of the Sheffield Sling Surgery due to friends attending and had contacted Rosie early on in pregnancy as I had planned to carry my baby in a sling. Once Alex was over the first big hurdle of coming off the ventilator at a month old, I got back in touch to find out if slings could help us while still in the NICU. The physiotherapist on the unit was very in favour of using slings and gave me a Vija top to try, but I felt it was more comfy just using my strappy top as we got so tangled with the wires.By the time we moved to HDU it was a slightly more relaxed environment with staff that seemed more in favour of breastfeeding and skin to skin. I decided, after discussion with Rosie, to buy my first sling, a Hana stretchy wrap.
I spent my time holding Alex as much as I could and when he was too poorly to be held I touched him through the incubator and spoke and sang to him. I felt being physically close would help us both bond better, especially after an awful pregnancy and so much separation. I was already aware of the Sheffield Sling Surgery due to friends attending and had contacted Rosie early on in pregnancy as I had planned to carry my baby in a sling. Once Alex was over the first big hurdle of coming off the ventilator at a month old, I got back in touch to find out if slings could help us while still in the NICU. The physiotherapist on the unit was very in favour of using slings and gave me a Vija top to try, but I felt it was more comfy just using my strappy top as we got so tangled with the wires.By the time we moved to HDU it was a slightly more relaxed environment with staff that seemed more in favour of breastfeeding and skin to skin. I decided, after discussion with Rosie, to buy my first sling, a Hana stretchy wrap.
It felt complicated at first getting used to the technique of wrapping and because of all the monitoring it would often take someone else to help me get all the wires sorted, but once Alex was put into the sling he fell straight to sleep. I noticed that often his heart rate and oxygen sats would improve too and it made me even more determined to keep him close.

Our journey through special care gives me mixed emotions. On the one hand I would never wish this experience on anyone. The constant stress, not just for myself but also family and friends around me. The fear that if I leave, something might happen. Every time the phone rang panic would set in and don't even get me started on the paediatricians coming up to the ward!
However, my life has changed completely in so many good ways. I have realised and experienced how fantastic the care is from my colleagues. I have become closer to my family and friends and I love watching my parents with Alex. I feel I will be an even more sympathetic and understanding midwife and I hope my practice will change to support women who go through similar experiences. Most of all I have realised my dream of becoming a mum and to the most incredible little fighter I have ever met.

I feel I have a strong bond with Alex and many people have commented on how well I can read him. I believe it is because of staying close to him as much as I have and having him in the sling has facilitated this.
Alex has Chronic Lung Disease and came home on oxygen in March. He is doing incredibly well on the lowest level now, but transporting the oxygen has been a bit of a challenge for me. The canister is heavy and the container rucksack has narrow shoulders so has hurt my shoulders; trying to balance that weight against Alex has not been easy. At times I have felt isolated simply because of that. However I have met some wonderful people on my journey through special care and in the sling community (often the two groups mix!) and we wouldn't be where we are now without these challenges.
We are still using our Hana wrap, and I've been trying out a snuggly Sleepy Nico! I've learned how to use woven wraps; we are beginning to back carry; the end of the oxygen is in sight! Time to tuck Alex up into the Sleepy Nico and reconnect after a long day.

Healthy Hips - busting some myths
Healthy Hips - this is a very common worry for parents who want to ensure they have the best information regarding their child's safety. Here, Rosie busts some of the myths and assesses what we really know on the subject.
People often ask me about the importance of a good position for their child’s hips in a carrier, having heard about “hip dysplasia” and “knee to knee”. These are good questions to consider, as there is a lot of hearsay and slightly misinformed information circulating around the internet.
I thought it would be helpful to discuss some common queries and consider what “best practice” might be. I will look at what hip dysplasia actually is and assess if narrow based carriers really are harmful to children. I will suggest some alternatives that are much more respectful of child anatomy and more comfortable for baby and parent.
1) What is hip dysplasia?
There are many terms used for this spectrum of related developmental hip problems in infants and children. These are often present at birth. Most recently the term “Developmental Hip Dysplasia” is being used, as there is evidence to suggest that while many hip disorders, (ranging from full dislocation, to unstable shallow sockets) are present at birth, some children with apparently normal hips go on to develop problems in the first year of life.
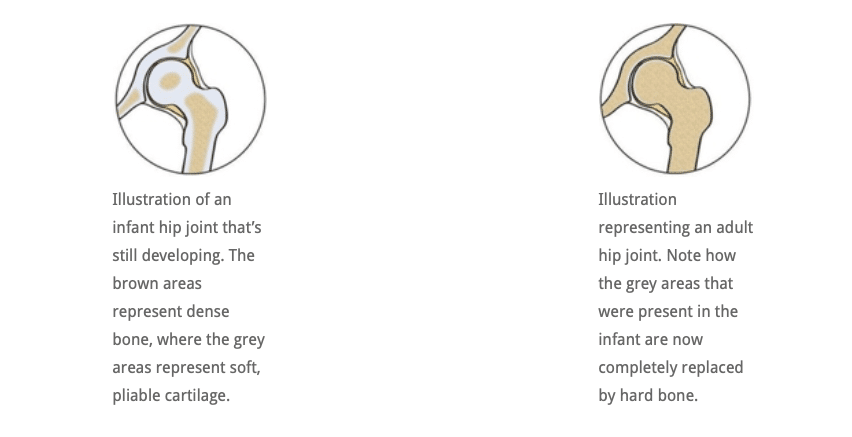
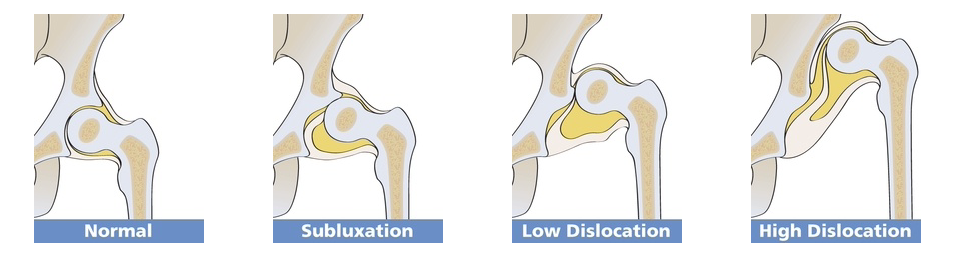
In simple terms, dysplasia means “growing abnormally”. Compared to adults, an infant’s hip sockets are made up of a greater proportion of softer, more pliable cartilage in relation to bone. This means that it is easier, anatomically, for the ball (the femoral head) to slip out of of the socket (the acetabulum) and be misaligned (subluxated) or fully dislocated. A normally formed hip joint will not encounter problems, but this softer structure, in combination with an abnormal socket shape, explains why some joints will dislocate.
In a child who has an abnormally developed hip joint, the combination of the shallow angle of the socket and the softer structure means that the ball (femoral head) is not held securely within the socket and can become misaligned and even slip out if the joint is placed under downward strain. If it does not slip back in, it is a dislocated joint and will need intervention. See the Hip Dysplasia website for more.

2) Is my child at risk of hip dysplasia?
The causes for hip dysplasia are poorly understood. There seems to be an increased risk if there is a positive family history of hip dysplasia. Female babies seem to be 4-5 times more at risk than males, and several factors in pregnancy seem to be relevant. For example,
- a tight uterus
- reduced uterine fluid that constricts the baby and prevents free fetal movement,
- breech delivery
- another condition that affects how babies lie in utero (such as fixed foot deformity)
all seem to be related to the presence of dysplasia. The left hip seems to be more frequently involved than the right. Furthermore, the growing baby is exposed to the mother’s oestrogen hormones. Oestrogen is thought to encourage ligament relaxation near the time of delivery, which may help with giving birth, but potentially may also cause the baby’s hip ligaments to be somewhat lax and increase the risk of an unstable joint.
These are not risks that a parent has any control over, clearly.
However, there are studies that strongly suggest that some cultures who swaddle their infants tightly (such as the Native American societies prior to the 1950’s, and some Japanese societies) have a far greater incidence of developmental hip dysplasia and childhood hip dislocation.
It is interesting to see that once the Najavo Indian culture, (who carried their babies tightly bound on cradle boards with their legs straightened ie extended and adducted), adopted bulky cloth nappies, the incidence of childhood hip dislocation decreased dramatically, even though they continued to use the cradle boards.
This was due to the nappies encouraging the babies’ legs to be held in a more natural flexed and abducted position (like a spread squat, as if child held on hip with legs around parent). African cultures, who do not swaddle their babies, and carry them constantly astride their backs from birth, have a very low incidence of hip dysplasia. You can read a very helpful scholarly article here for more information.
In 2015 the Journal of Paediatric Orthopaedics published an article based on data from 40,000 children in Malawi and a systematic review of current evidence. “The majority of mothers in Malawi back-carry their infants during the first 2 to 24 months of life, in a position that is similar to that of the Pavlik harness. We believe this to be the prime reason for the low incidence of DDH in the country. In addition, there is established evidence indicating that swaddling, the opposite position to back-carrying, causes an increase in the incidence of DDH. If a carrying position of infants during their early months of development can reduce the incidence of DDH, then a public health initiative promoting back carrying could have significant world health and financial implications in the future management of DDH and also have potentially huge effects on the timing and severity of development of adult hip arthritis.”
“Hence it appears logical to discourage putting the baby’s legs in the extended position, and encourage keeping the baby’s hips spread apart. This latter position places the head of the femur (the ball) against the acetabulum (the socket), and encourages deepening of the socket.” (Quote from Orthoseek– a source of authoritative information on paediatric orthopaedics.)
So, a parent can potentially reduce the small risk of hip dysplasia by carefully considering some of the practices they adopt.
3) How is hip dysplasia diagnosed and treated?
Diagnosis: Most suspected cases of hip dysplasia are picked up at birth or at the six week check, by physical examination, but some cases are missed, sometimes with significant consequences. There is a strong case for routine ultrasound screening for hip dysplasia, as comprehensive ultrasound screening during the immediate newborn period has demonstrated hip laxity in approximately 15% of infants (Rosendahl K, et al. Pediatrics 1994;94:47-52)
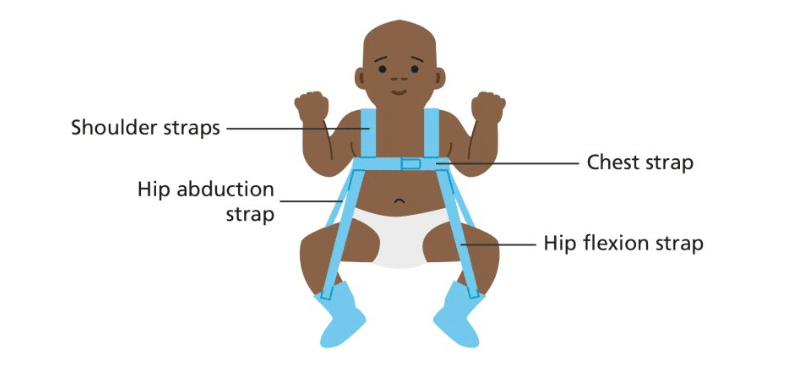
Treatment: Mild cases can be managed by “double diapering” to keep hips in the flexed, abducted spread squat position. More severe cases may need splinting with a Pavlik harness and sometimes surgery is required. Many children respond very well to this and lead normal lives. If left untreated, and picked up later in childhood (eg a limp) developmental hip dysplasia can have chronic consequences, such differences in leg length, awkward gaits or decreased agility. Older children may even develop early arthritis of the hip. Sometimes complex surgery is needed.
4) Is there anything I can do to reduce my child’s chance of hip problems?
It isn’t fully clear exactly how large a role the choices parents make (eg swaddling, cloth nappy use, carrying in an appropriate sling) have on the likelihood of hip problems later in life. Some babies may have mild DDH at birth that is not discovered at all, and thus unwittingly benefit from good hip positioning that a wider based carrier gives, encouraging the mild laxity to self-correct. There are many cases of babies who have been found to have DDH and been advised to use a wider based carrier by their orthopaedist, and the shallowness has self corrected. Clearly, wider based carriers are beneficial.
Furthermore, by 6 months of age, the risk of hip dysplasia has largely passed, and by one year children are stronger, better developed, and able to place their hips in a healthy position themselves when required for comfort (ie pull their knees up or ask to get down), so older children are not at risk. It is young babies in the first few months of life that need more caution.
2018 update. There has been a small increase in the late diagnosis of DDH, which is thought to be possibly related to the use of tight swaddling, a technique to settle babies that has seen some resurgence recently. Firm swaddling of the lower body forces babies’ legs into prolonged positions of tight adduction and extension which can be damaging to hips that are already vulnerable. Swaddling should always be done in a hip healthy way (read more here about the late diagnosis of DDH).
It would seem sensible, therefore, at least in the early months of life, to encourage babies and small children to have their hips held in a healthy position, that is less likely to place strain on lax ligaments or possibly shallow hip sockets. A good, wide-based sling or carrier can assist with this healthy hip position. This will also be more comfortable for the child – consider perching on or astride a stool versus sitting on a chair or even in a hammock!
It is worth being aware that there is often variance in the advice orthopaedic surgeons offer, based on their depth of knowledge of babywearing. There is little formal research on the effects of slings per se in children with DDH, and much is extrapolated. The Institute of Hip Dysplasia is a helpful resource.
2024 update. There has been a lot of interest in the possibility of using cloth nappies to keep children’s hips in a wider based position. Evidence that this is helpful is lacking. This may prove a useful read, a study done into this very thing. It does recommend slings and carriers!
5) Will my narrow-based high-street carrier harm my baby’s hips?
Much debate has been held on the role that narrow -based carriers may have on the worsening of pre-existing, undiagnosed hip dysplasia, or promoting its development in normal hips. It is worth bearing in mind that few parents use narrow based carriers for any significant length of time, as they are often not especially comfy, and babies’ legs are free to move in the carrier, rather than being held forcibly in one position. Many narrow based carriers are wider than they used to be, so small babies often end up in a slightly abducted and rotated position anyway.
So the simple answer to the question is “Probably not, in the majority of cases.” This assumes your child’s hips are normal, and they are not one of the postulated 15% of infants whose condition is missed by health care professionals (however well-meaning). These children will most certainly benefit from a wider based carrier.
So you are unlikely to damage your child’s hips if they are healthy. It will be up to you to assess the risk that mild DDH may not have been identified at the routine screening, and make the choice for yourself.
These narrow based carriers usually have a particular feature of robust head and neck support. The reason for this is because a child who has unsupported legs will usually end up with an arched, over-straightened spine where their head and airway is not adequately protected. Baby’s heavy head is more likely to fall backwards, and therefore rigid neck supports are needed to keep him safe. This is in contrast witih carrying positions which do encourage the natural pelvic tuck and therefore a curved spine and baby’s head becoming self-supporting while he rests against parent (think about how you often only need to support baby’s bottom when they are sleeping on your chest or shoulder).

Parents of children with normal, non-dysplastic joints are unlikely to “cause” hip dysplasia by choosing to use one of these narrow-based slings, but these designs do not, on the whole, promote the flexed, abducted spread-squat position that seems to encourage better hip joint positioning and deeper development of the socket. A sling that supports baby’s thighs from beneath (“knee to knee”) is more likely to keep hips in this optimal position, and reduce strain on still-developing joints. It is interesting to note that the bigger brands who are well known for making narrow based carriers have begun to redesign their products to be more broad at the base and more respectful to baby anatomy.
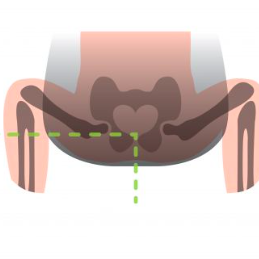
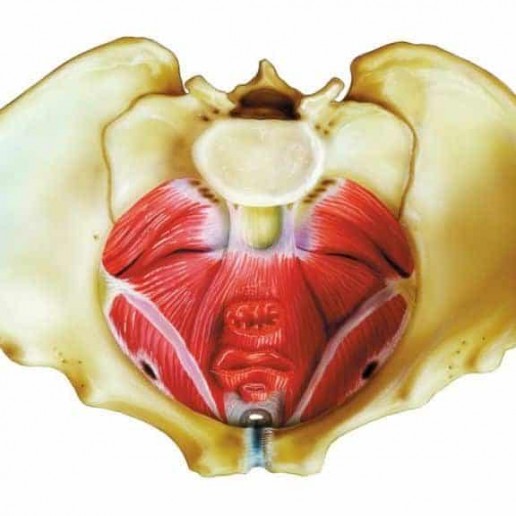
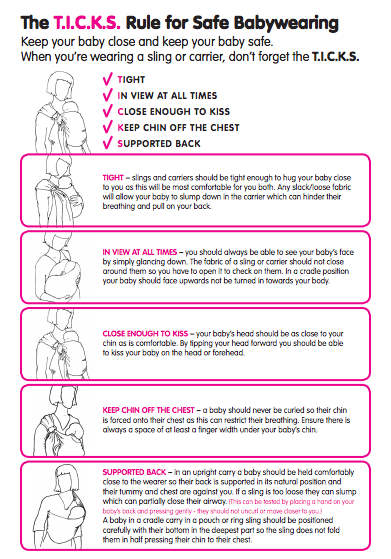
It will be no surprise then, that most professionally-trained babywearing consultants will advocate the thighs being supported right into the knee pits into an M shape, with knees held higher than the bottom (nearer to an imaginary horizontal line out from the belly button). This puts the femoral head into an ideal central position in the socket, and is the position adopted by the Pavlik Harness as you can see above.
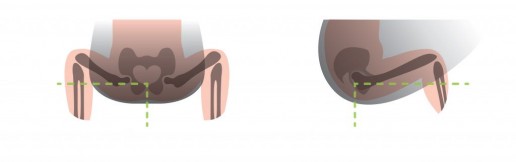
Here is are some drawings that show the most typically seen position in a narrow based carrier, and then the ideal hip position in a sling
1) Classic high-street narrow-based carrier (red arrows). The legs are hanging downwards, entirely unsupported. The infantile hip-socket is taking the full weight of the legs and there will be a lot of unhelpful strain. It is similar to balancing on a beam at the gym with all the weight being borne on a narrow strap between the legs. Baby’s back may be straightened, meaning their head is able to fall backwards, needing rigid head and neck support.
2) A properly fitting, wide-based carrier (green arrows). Observe the M-shape that has been created, with the thighs securely supported all the way to the knees, which are held above the bottom. The hip joints are in the optimal position, and there is no weight at all dragging down on the joint. Orthopaedic consultants recommend thighs to be resting at an angle of 100 degrees from the midline.

These drawings show how there is no downward strain on the socket and the child is supported widely across a large proportion of their base. The baby is clearly seated comfortably with their weight widely distributed, and the gentle curve of their spine protected. This baby’s upper body will be supported against the parent with head resting on parent’s chest, and rigid head supports are not needed (using natural anatomical positions).
6) What slings would you recommend for healthy hip position?
All safe babywearing is to be celebrated and encouraged! Using a narrow-based carrier will not harm the majority of children (see above), so if you have one already, there are a few things you can do to improve your child’s comfort such as using a scarf tucked into the seat, as in this video. This will encourage a change of position from legs hanging straight downwards (extended and adducted) to supported knee to knee (flexed and abducted) in the M shape, as discussed above. It is, however, only a temporary solution – I would advise you to use a wider-based carrier.
To reproduce the hip-healthy M shape, when putting a child into a carrier, tilt their pelvises inwards slightly and push the feet below their bent knees upwards to encourage flexion. All babies are different, and some will naturally spread their legs more widely than others. NEVER force your baby’s legs to move into a position that does not come easily.
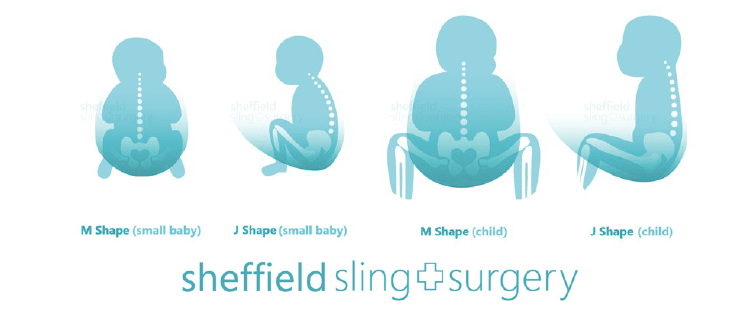
If you don’t yet have a sling for your baby, go for a soft one that is well designed to both promote healthy hip M-position and encourage the natural gently curved J-spine shape that young children have (rather than a tight C shape where a heavy head would be drooping down onto the chin curled over). The secondary curves begin to develop later on in life – the cervical curve when they gain head control and can lift against gravity, and the lumbar curve at the crawling/walking stage . Until then, spines should not be artificially kept straight (ie babies should avoid too much time in rigid car seats, stiff inflexible carriers, or lying supine on their backs).
It is worth remembering that well-designed slings that focus on supporting a child’s legs and curved spine can be used in a less than ideal way. It is possible to use a good tool in a less than optimum manner, especially when in a hurry, so it is worth taking your time to position the sling well and to be actively aware of your child’s hip and spine positions when putting the sling on.
Examples of suitable slings (this list is not exhaustive and is merely a guide). See your local sling meet/consultant/library for more help and advice or read our sling guide.
Stretchy wraps, Close Carrier hybrid
Ring slings or Scootababy hip carrier
Meh Dais and Half-Buckles and variants
7) What do I do when my child’s legs are too long for “knee to knee” support?
Small babies, sadly, all too soon grow into big babies, with longer legs, and can start to out-grow their slings in terms of thigh support along to the knees. And then they start to toddle! When a child can stand unaided and walk, he will have the muscle and ligament strength to bear the weight of his own legs well, so full knee-to-knee is less important for toddlers, but for smaller babies, helping to support their legs is important. You may need a wider sling, or you can adjust the one you have already with a helpful scarf – there is a great video here from Slingababy.
8) Where can I find more help and support and reading about using a sling for my child?
There are numerous resources in the UK where you can get babywearing advice and encouragement, such as your local babywearing consultant, sling meet, or sling library. The links below will help (again, not an exhaustive list!)
The Carrying Matters Sling Guide
Dr E Kirklionis’ book A Baby Wants to Be Carried is highly recommended, for its overview of the evolutionary theory behind baby carrying and the spread squat positioning.
You can read my book Why Babywearing Matters too
Hip Dysplasia Institute statement on babywearing and Hip Healthy status

Blog
The Carrying Matters blog page.. enjoy reading! If you have any topics you'd like to see covered, get in touch! I enjoy writing and am always keen to hear of new ideas, and to host guest blog posts too!































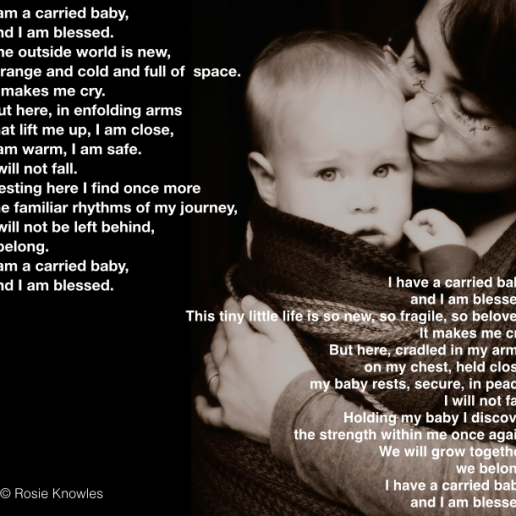
I am a Carried Baby
Why do we carry our babies? We carry them because it is a biological, instinctive parental response, that blesses the children we carry, and that blesses us. I find myself blessed by the small part I…
Can I carry my baby in a sling if I have epilepsy?
Guest Blog from a friend of mine about her choice to use a sling to keep her child close despite her diagnosis of epilepsy. It has worked out very well for her. Here she discusses the processes of…

Breast and Bottle Feeding Safely in a Sling
I meet a lot of pregnant ladies in the course of my varied roles, and many new mums, and one of the questions I am most frequently asked is "Will I be able to feed my baby in a sling?" It's an…
The unhelpful "rules" of babywearing
There are so many unhelpful rules of babywearing. I'm not talking about basic safety guidelines, but about the unspoken rules about how things must be done.This needs addressing. I love babywearing. I love how special it is. I love how empowering and enabling it can be and what a difference it can make to children and their carers and the society around them.
I also love that it just makes life work for so many people on a practical level, regardless of all the benefits and reasons about why it is an activity that matters. Babywearing may be magical for many, and has so many positive effects on a physiological and neurological level, but really, for some, it’s just about getting stuff done, keeping the cogwheels of daily life turning, or helping to survive very tough situations.
I have watched thousands of people carrying their children all around the world and I love that I am part of a tradition of child rearing that goes back beyond the history books into our anthropological origins. I love it so much that I wrote a book all about it!

Carrying children is normal human behaviour, and it isn’t, and shouldn’t be, complicated or difficult. It shouldn’t be scary, inaccessible or expensive. It does not belong to groups of people to “own” or to build tall walls around to make things secret or elitist. Babywearing (the use of a sling or carrier to keep a child safe and close to a parent) is for everyone, every gender, every colour, every ability, every size, every shape. Babywearing should bring us together, not divide us. It should not alienate or exclude entire groups of people.
However, as the practice becomes more mainstream and the industry grows, this alienation is unfortunately happening more and more often. Marketing campaigns and the general make-up of many babywearing groups suggests that this is an activity for relatively well-off middle class “standard sized” white women in nuclear families, carrying able-bodied and healthy children. This is a direction that needs to be arrested before it becomes too entrenched. I’ll say it again, babywearing is for everyone and can be done in so many ways.




One way that babywearing can become elitist is in the development of complex rules, and I’d like to have a discussion about some of these “rules” and “guides” of babywearing that I am seeing shared around. I understand that it can feel reassuring to have black and white lists of what you can and can’t do, and schedules for certain types of carrying. These can act as a framework for where to begin with using a sling. This is valuable, especially as many of us have lost the shared collective wisdom that comes from living in communities and no longer learn how to parent from the people living around us. Many of us turn to books and to the internet and ask for guidance.
However, I think these “rules” often end up making things harder and disempowering the very people who need the most support. Here are some common examples.
Some commonly stated "Rules"
- Do not use a stretchy wrap beyond three months
- Do not back carry with a stretchy wrap
- Do not use a soft structured carrier for a newborn
- Do not do any form of sideways cradle carry
- Do not use a narrow based carrier
- Do not face your child out in a carrier
- Do not back carry a baby before they can sit unaided
- Do not back carry a newborn in a ring sling
- Low back carries are dangerous, high back carries are much better
- Once your baby is walking you must begin to use a toddler-size carrier
- Bigger children must be carried on the back
- Do not use footed pyjamas for babies in slings
I could go on…
These rules can be useful, but often they exclude significant proportions of the population. You can use a stretchy wrap to carry an older child, if they are safe and comfy. You can use your stretchy wrap in many ways, including on the back, if your child is safe and comfy. You can use a soft structured carrier for a newborn, if it fits them and is safe and comfy. You can carry a child in a sideways seated position or even a cradle carry, and facing out, if they are safe and comfy. You can use a narrow based carrier for a baby or a baby sized carrier for a toddler, if they are safe and comfy. You can carry a baby on your back in any form of carrier if they are safe and comfy. You can carry any age baby on your back or your front if they are safe and comfy. You can carry your child who is wearing footed pyjamas if the child is safe and comfy (ie their toes have room to wiggle). You can carry your child whatever size you are. In fact, you can do pretty much anything you want to do, if your baby is safe and comfy.
Do you get the theme?
I think the only “rules” when it comes to carrying a child in any form of sling are
- Can they breathe safely and without any obstruction at all times?
- Are they being held safely and securely in a carrier that fits (to ensure they are able to breathe easily and cannot slump into a position that would obstruct their airway)?
- Are they as comfortable as the circumstances allow?
How do you check if a child is breathing safely in the carrier?
- Look at them, listen to them, be aware of them.
- Check their airways are free of any fabric and they are not slumping or folded over with their ribcage compressed and chin on the chest.
How do you ensure they are safe and snug in the carrier and that it fits?
- A well fitting carrier holds a child close to the parent, close enough that if the parent leans forwards, the child does not swing free. This helps to avoid slumping over in the carrier.
- If a child’s body can slump, the carrier does not fit or is not tight enough.
- The “knee to knee” rule is often overstated in its importance for older children (the M shape can be protective for children at risk of hip dysplasia in the early months.)
How do you ensure they are comfortable in the carrier?
- This is all about being responsive and connected to the child being carried.
- They should fit inside the carrier, be able to breathe safely, and should not be too hot (overheated babies are more likely to stop breathing).
- Check on your child, be aware of their experience and how they are behaving in the carrier. The more you interact with your child the more you will know that they are OK (or not!)
If your baby is safe, able to breathe and is comfortable, and you feel confident that all is well, then it probably is well. Carry right on! And if you would like some encouragement, find a friendly educator and help them learn how to support you in a way that builds you up and keeps you carrying happily.
It is important to remember that every child and every parent has different needs. Parents of twins may need to be able to back carry one twin from a very early age, to be able to cope with family life. They may choose to use a buckle carrier on the back, and if the child is able to breathe safely and is not uncomfortable then that makes their lives work. Telling them this is forbidden creates needless barriers and makes life harder. A stretchy wrap for a one year old may not be as comfortable as a woven wrap, but for a parent on a budget who now has a less-unhappy toddler held close while the baby can be cleaned, this is a win-win situation. A four month old who will will only tolerate facing out in a narrow based carrier can be happily transported on a school run. Millions of women around the world have carried young babies in low torso carries with simple pieces of cloth. A disabled child who cannot sit unaided can be held safely and securely on the back in several types of carrier which will definitely make everything much easier. Do be aware of how your language and how you educate can affect others and significantly disempower people.
“Oh, but these rules are for normal people!” This is a common dismissal of any criticism of “rules” and is unbelievably inappropriate. Our society is made up of people of all abilities and all skills. More than one billion people in today’s world have a disability; that’s 15% of the population. This ratio may not be reflected in the proportion of children who are brought to babywearing groups, just like people of colour are missing from these gatherings. The fault is not theirs; it is ours. We must be more inclusive and we must make efforts to reach out to people. Just imagine how different things could be, if some of these walls of prejudice were pulled down from the inside.
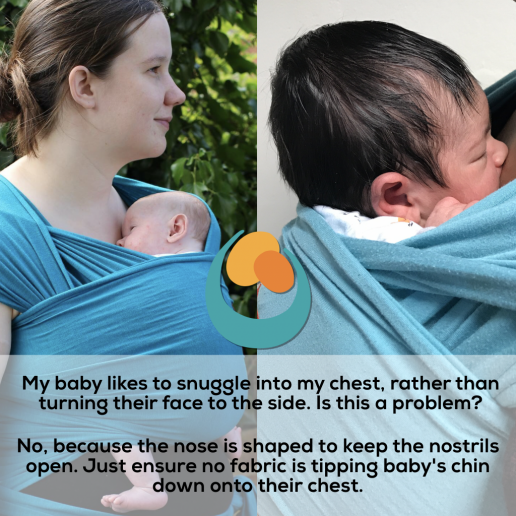
Grainne and Tessa are a great example of how babywearing can actually empower beyond the “rules.” Little Tessa was born without a nose (arhinia) and had to have a tracheostomy when she was very young. Her family were told that she was safest to be sleeping in a separate room with various wires and monitors attached to her for any alerts in a change of breathing. In fact, Grainne decided to wear Tessa in a sling, keeping her close and safe and visible at all times; if Tessa stopped breathing, Grainne would see it and feel it as it happened, thanks to the sling (read more about them here.) The sling made life work for them, and also made it much happier during some very tough times. Common sense, knowledge of safety and a willingness to bend the rules worked together to enhance their lives, when they could so easily have missed out.


This is a superb blog for further reading; all about ableism in the babywearing community and I urge you to read it.
http://bindungtraegt.de/ableismback-wearing/
Please also read the Tania Talks blog posts on babywearing (she is a wheelchair user)
https://www.whentaniatalks.com/the-realities-of-back-carrying-as-a-wheelchair-user/
https://www.whentaniatalks.com/back-carrying-as-a-wheelchair-user/