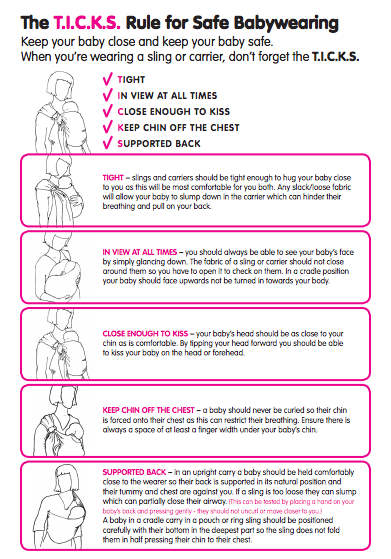
Healthy Hips - busting some myths
Healthy Hips - this is a very common worry for parents who want to ensure they have the best information regarding their child's safety. Here, Rosie busts some of the myths and assesses what we really know on the subject.
People often ask me about the importance of a good position for their child’s hips in a carrier, having heard about “hip dysplasia” and “knee to knee”. These are good questions to consider, as there is a lot of hearsay and slightly misinformed information circulating around the internet.
I thought it would be helpful to discuss some common queries and consider what “best practice” might be. I will look at what hip dysplasia actually is and assess if narrow based carriers really are harmful to children. I will suggest some alternatives that are much more respectful of child anatomy and more comfortable for baby and parent.
1) What is hip dysplasia?
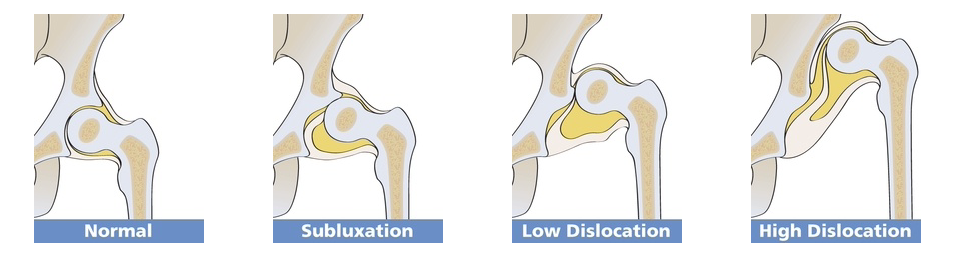
There are many terms used for this spectrum of related developmental hip problems in infants and children. These are often present at birth. Most recently the term “Developmental Hip Dysplasia” is being used, as there is evidence to suggest that while many hip disorders, (ranging from full dislocation, to unstable shallow sockets) are present at birth, some children with apparently normal hips go on to develop problems in the first year of life.
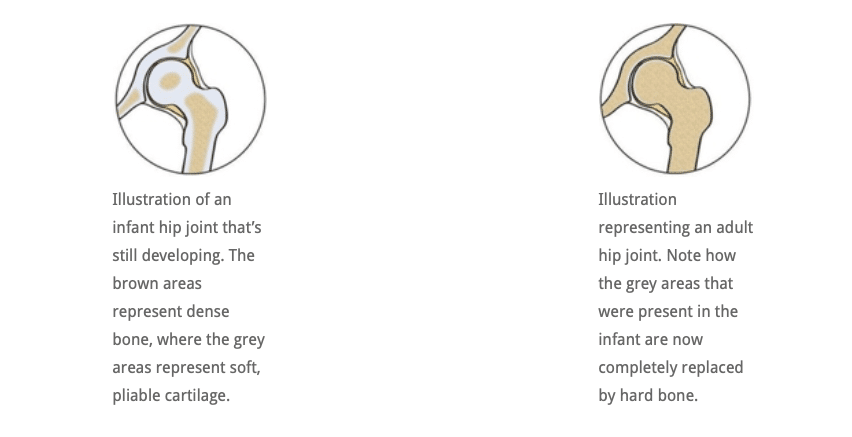
In simple terms, dysplasia means “growing abnormally”. Compared to adults, an infant’s hip sockets are made up of a greater proportion of softer, more pliable cartilage in relation to bone. This means that it is easier, anatomically, for the ball (the femoral head) to slip out of of the socket (the acetabulum) and be misaligned (subluxated) or fully dislocated. A normally formed hip joint will not encounter problems, but this softer structure, in combination with an abnormal socket shape, explains why some joints will dislocate.
In a child who has an abnormally developed hip joint, the combination of the shallow angle of the socket and the softer structure means that the ball (femoral head) is not held securely within the socket and can become misaligned and even slip out if the joint is placed under downward strain. If it does not slip back in, it is a dislocated joint and will need intervention. See the Hip Dysplasia website for more.

2) Is my child at risk of hip dysplasia?
The causes for hip dysplasia are poorly understood. There seems to be an increased risk if there is a positive family history of hip dysplasia. Female babies seem to be 4-5 times more at risk than males, and several factors in pregnancy seem to be relevant. For example,
- a tight uterus
- reduced uterine fluid that constricts the baby and prevents free fetal movement,
- breech delivery
- another condition that affects how babies lie in utero (such as fixed foot deformity)
all seem to be related to the presence of dysplasia. The left hip seems to be more frequently involved than the right. Furthermore, the growing baby is exposed to the mother’s oestrogen hormones. Oestrogen is thought to encourage ligament relaxation near the time of delivery, which may help with giving birth, but potentially may also cause the baby’s hip ligaments to be somewhat lax and increase the risk of an unstable joint.
These are not risks that a parent has any control over, clearly.
However, there are studies that strongly suggest that some cultures who swaddle their infants tightly (such as the Native American societies prior to the 1950’s, and some Japanese societies) have a far greater incidence of developmental hip dysplasia and childhood hip dislocation.
It is interesting to see that once the Najavo Indian culture, (who carried their babies tightly bound on cradle boards with their legs straightened ie extended and adducted), adopted bulky cloth nappies, the incidence of childhood hip dislocation decreased dramatically, even though they continued to use the cradle boards.
This was due to the nappies encouraging the babies’ legs to be held in a more natural flexed and abducted position (like a spread squat, as if child held on hip with legs around parent). African cultures, who do not swaddle their babies, and carry them constantly astride their backs from birth, have a very low incidence of hip dysplasia. You can read a very helpful scholarly article here for more information.
In 2015 the Journal of Paediatric Orthopaedics published an article based on data from 40,000 children in Malawi and a systematic review of current evidence. “The majority of mothers in Malawi back-carry their infants during the first 2 to 24 months of life, in a position that is similar to that of the Pavlik harness. We believe this to be the prime reason for the low incidence of DDH in the country. In addition, there is established evidence indicating that swaddling, the opposite position to back-carrying, causes an increase in the incidence of DDH. If a carrying position of infants during their early months of development can reduce the incidence of DDH, then a public health initiative promoting back carrying could have significant world health and financial implications in the future management of DDH and also have potentially huge effects on the timing and severity of development of adult hip arthritis.”
“Hence it appears logical to discourage putting the baby’s legs in the extended position, and encourage keeping the baby’s hips spread apart. This latter position places the head of the femur (the ball) against the acetabulum (the socket), and encourages deepening of the socket.” (Quote from Orthoseek– a source of authoritative information on paediatric orthopaedics.)
So, a parent can potentially reduce the small risk of hip dysplasia by carefully considering some of the practices they adopt.
3) How is hip dysplasia diagnosed and treated?
Diagnosis: Most suspected cases of hip dysplasia are picked up at birth or at the six week check, by physical examination, but some cases are missed, sometimes with significant consequences. There is a strong case for routine ultrasound screening for hip dysplasia, as comprehensive ultrasound screening during the immediate newborn period has demonstrated hip laxity in approximately 15% of infants (Rosendahl K, et al. Pediatrics 1994;94:47-52)
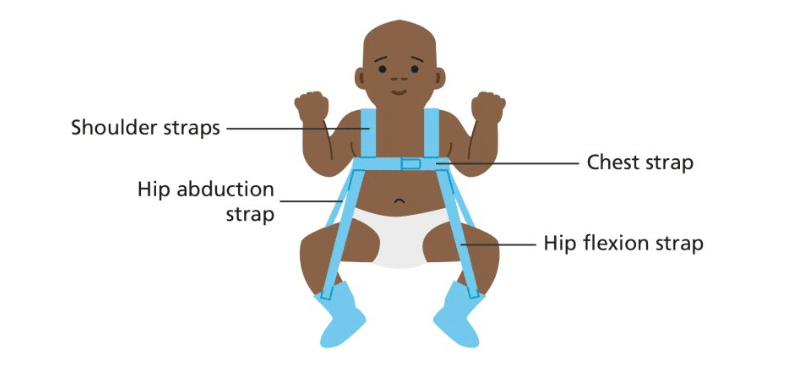
Treatment: Mild cases can be managed by “double diapering” to keep hips in the flexed, abducted spread squat position. More severe cases may need splinting with a Pavlik harness and sometimes surgery is required. Many children respond very well to this and lead normal lives. If left untreated, and picked up later in childhood (eg a limp) developmental hip dysplasia can have chronic consequences, such differences in leg length, awkward gaits or decreased agility. Older children may even develop early arthritis of the hip. Sometimes complex surgery is needed.
4) Is there anything I can do to reduce my child’s chance of hip problems?
It isn’t fully clear exactly how large a role the choices parents make (eg swaddling, cloth nappy use, carrying in an appropriate sling) have on the likelihood of hip problems later in life. Some babies may have mild DDH at birth that is not discovered at all, and thus unwittingly benefit from good hip positioning that a wider based carrier gives, encouraging the mild laxity to self-correct. There are many cases of babies who have been found to have DDH and been advised to use a wider based carrier by their orthopaedist, and the shallowness has self corrected. Clearly, wider based carriers are beneficial.
Furthermore, by 6 months of age, the risk of hip dysplasia has largely passed, and by one year children are stronger, better developed, and able to place their hips in a healthy position themselves when required for comfort (ie pull their knees up or ask to get down), so older children are not at risk. It is young babies in the first few months of life that need more caution.
2018 update. There has been a small increase in the late diagnosis of DDH, which is thought to be possibly related to the use of tight swaddling, a technique to settle babies that has seen some resurgence recently. Firm swaddling of the lower body forces babies’ legs into prolonged positions of tight adduction and extension which can be damaging to hips that are already vulnerable. Swaddling should always be done in a hip healthy way (read more here about the late diagnosis of DDH).
It would seem sensible, therefore, at least in the early months of life, to encourage babies and small children to have their hips held in a healthy position, that is less likely to place strain on lax ligaments or possibly shallow hip sockets. A good, wide-based sling or carrier can assist with this healthy hip position. This will also be more comfortable for the child – consider perching on or astride a stool versus sitting on a chair or even in a hammock!
It is worth being aware that there is often variance in the advice orthopaedic surgeons offer, based on their depth of knowledge of babywearing. There is little formal research on the effects of slings per se in children with DDH, and much is extrapolated. The Institute of Hip Dysplasia is a helpful resource.
2024 update. There has been a lot of interest in the possibility of using cloth nappies to keep children’s hips in a wider based position. Evidence that this is helpful is lacking. This may prove a useful read, a study done into this very thing. It does recommend slings and carriers!
5) Will my narrow-based high-street carrier harm my baby’s hips?
Much debate has been held on the role that narrow -based carriers may have on the worsening of pre-existing, undiagnosed hip dysplasia, or promoting its development in normal hips. It is worth bearing in mind that few parents use narrow based carriers for any significant length of time, as they are often not especially comfy, and babies’ legs are free to move in the carrier, rather than being held forcibly in one position. Many narrow based carriers are wider than they used to be, so small babies often end up in a slightly abducted and rotated position anyway.
So the simple answer to the question is “Probably not, in the majority of cases.” This assumes your child’s hips are normal, and they are not one of the postulated 15% of infants whose condition is missed by health care professionals (however well-meaning). These children will most certainly benefit from a wider based carrier.
So you are unlikely to damage your child’s hips if they are healthy. It will be up to you to assess the risk that mild DDH may not have been identified at the routine screening, and make the choice for yourself.
These narrow based carriers usually have a particular feature of robust head and neck support. The reason for this is because a child who has unsupported legs will usually end up with an arched, over-straightened spine where their head and airway is not adequately protected. Baby’s heavy head is more likely to fall backwards, and therefore rigid neck supports are needed to keep him safe. This is in contrast witih carrying positions which do encourage the natural pelvic tuck and therefore a curved spine and baby’s head becoming self-supporting while he rests against parent (think about how you often only need to support baby’s bottom when they are sleeping on your chest or shoulder).

Parents of children with normal, non-dysplastic joints are unlikely to “cause” hip dysplasia by choosing to use one of these narrow-based slings, but these designs do not, on the whole, promote the flexed, abducted spread-squat position that seems to encourage better hip joint positioning and deeper development of the socket. A sling that supports baby’s thighs from beneath (“knee to knee”) is more likely to keep hips in this optimal position, and reduce strain on still-developing joints. It is interesting to note that the bigger brands who are well known for making narrow based carriers have begun to redesign their products to be more broad at the base and more respectful to baby anatomy.
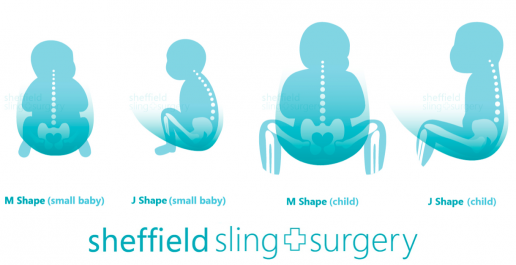
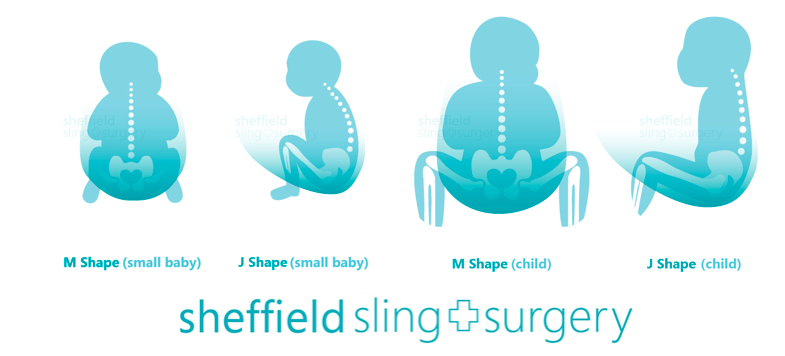
It will be no surprise then, that most professionally-trained babywearing consultants will advocate the thighs being supported right into the knee pits into an M shape, with knees held higher than the bottom (nearer to an imaginary horizontal line out from the belly button). This puts the femoral head into an ideal central position in the socket, and is the position adopted by the Pavlik Harness as you can see above.
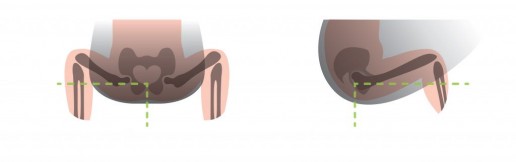
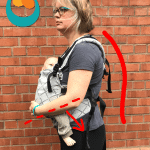
Here is are some drawings that show the most typically seen position in a narrow based carrier, and then the ideal hip position in a sling
1) Classic high-street narrow-based carrier (red arrows). The legs are hanging downwards, entirely unsupported. The infantile hip-socket is taking the full weight of the legs and there will be a lot of unhelpful strain. It is similar to balancing on a beam at the gym with all the weight being borne on a narrow strap between the legs. Baby’s back may be straightened, meaning their head is able to fall backwards, needing rigid head and neck support.
2) A properly fitting, wide-based carrier (green arrows). Observe the M-shape that has been created, with the thighs securely supported all the way to the knees, which are held above the bottom. The hip joints are in the optimal position, and there is no weight at all dragging down on the joint. Orthopaedic consultants recommend thighs to be resting at an angle of 100 degrees from the midline.

These drawings show how there is no downward strain on the socket and the child is supported widely across a large proportion of their base. The baby is clearly seated comfortably with their weight widely distributed, and the gentle curve of their spine protected. This baby’s upper body will be supported against the parent with head resting on parent’s chest, and rigid head supports are not needed (using natural anatomical positions).
6) What slings would you recommend for healthy hip position?
All safe babywearing is to be celebrated and encouraged! Using a narrow-based carrier will not harm the majority of children (see above), so if you have one already, there are a few things you can do to improve your child’s comfort such as using a scarf tucked into the seat, as in this video. This will encourage a change of position from legs hanging straight downwards (extended and adducted) to supported knee to knee (flexed and abducted) in the M shape, as discussed above. It is, however, only a temporary solution – I would advise you to use a wider-based carrier.
To reproduce the hip-healthy M shape, when putting a child into a carrier, tilt their pelvises inwards slightly and push the feet below their bent knees upwards to encourage flexion. All babies are different, and some will naturally spread their legs more widely than others. NEVER force your baby’s legs to move into a position that does not come easily.
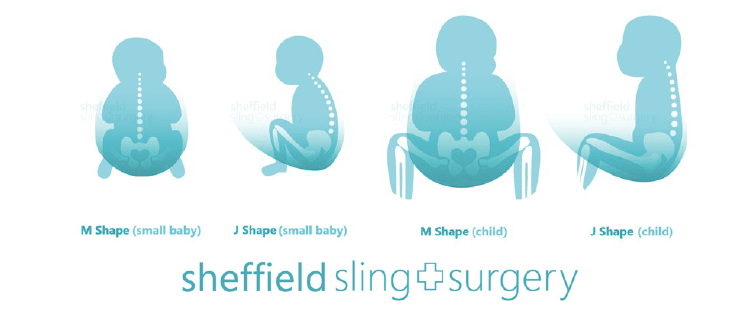
If you don’t yet have a sling for your baby, go for a soft one that is well designed to both promote healthy hip M-position and encourage the natural gently curved J-spine shape that young children have (rather than a tight C shape where a heavy head would be drooping down onto the chin curled over). The secondary curves begin to develop later on in life – the cervical curve when they gain head control and can lift against gravity, and the lumbar curve at the crawling/walking stage . Until then, spines should not be artificially kept straight (ie babies should avoid too much time in rigid car seats, stiff inflexible carriers, or lying supine on their backs).
It is worth remembering that well-designed slings that focus on supporting a child’s legs and curved spine can be used in a less than ideal way. It is possible to use a good tool in a less than optimum manner, especially when in a hurry, so it is worth taking your time to position the sling well and to be actively aware of your child’s hip and spine positions when putting the sling on.
Examples of suitable slings (this list is not exhaustive and is merely a guide). See your local sling meet/consultant/library for more help and advice or read our sling guide.
Stretchy wraps, Close Carrier hybrid
Ring slings or Scootababy hip carrier
Meh Dais and Half-Buckles and variants
7) What do I do when my child’s legs are too long for “knee to knee” support?
Small babies, sadly, all too soon grow into big babies, with longer legs, and can start to out-grow their slings in terms of thigh support along to the knees. And then they start to toddle! When a child can stand unaided and walk, he will have the muscle and ligament strength to bear the weight of his own legs well, so full knee-to-knee is less important for toddlers, but for smaller babies, helping to support their legs is important. You may need a wider sling, or you can adjust the one you have already with a helpful scarf – there is a great video here from Slingababy.
8) Where can I find more help and support and reading about using a sling for my child?
There are numerous resources in the UK where you can get babywearing advice and encouragement, such as your local babywearing consultant, sling meet, or sling library. The links below will help (again, not an exhaustive list!)
The Carrying Matters Sling Guide
Dr E Kirklionis’ book A Baby Wants to Be Carried is highly recommended, for its overview of the evolutionary theory behind baby carrying and the spread squat positioning.
You can read my book Why Babywearing Matters too
Hip Dysplasia Institute statement on babywearing and Hip Healthy status

Troubleshooting your buckle carrier
Want to make the most of your buckle carrier and ensure it is as comfy for you and your child as possible? Here are some troubleshooting handy tips to help!
Before you start, check your carrier over for wear and tear, ensure the buckles aren’t broken, loosen any webbing that was left tightened, prepare anything that needs pre-clipping etc. Make sure your carrier is the right size for your baby.
Work on your waistband
- Choose where to place your waistband. This will depend in part on the length of your baby’s torso (the top of their head should be at least close enough to kiss, for airway protection. or higher). This may mean you need to wear the waistband quite high when your baby is small, as free airflow is vital. As they grow longer, the waistband can move further down your body!
- Waistband-less carriers (for example, the Integra) are positioned mainly for baby’s height and may need to be quite high for little babies as their bottoms sit lower than the webbing waist.
- Some people like to have the padded waistband right around their natural waist. If it is a wide or stiff band, try to have the lower end at least skimming over the top of your pelvic crests, rather than sitting on top, which may make it more comfortable.

- Some people find placing the padded waistband around the upper part of the pelvis helpful; this means that the weight does not rest on top of the pelvic crest and the waistband won’t dig in. Too low down may make it hard to walk. Try a few heights out!

- As your child grows your waistband is likely to need to move further down your body (which will also help you to see over your child’s head!)
- Make sure your waistband sits parallel to the floor rather than tipping forwards to be lower at the front. This distributes weight more evenly.

- The waistband does not need to be super tight; it just needs to be secure so it doesn’t slip.
- Ensure the buckle is fully clicked together.
- This post about babywearing with a weakened pelvic floor is worth a read, it shows some very helpful images of posture.


Practice your position
- Hold your child in the ergonomic M and J shaped position you are hoping to achieve, in the location on your body you wish them to be. It is worth taking the time to do this; it is much easier to bring the panel up over a well positioned child at the right height, rather than having to do a lot of fiddling or adjusting later. Their chest should be close to you, chin off their chest, with no slumping over. (see more here)

- It helps to have your child’s bottom a finger-breadth above the padded waistband. This will help to ensure the panel does not get bunched up underneath baby, which will shorten the panel. (Of course, if you are shortening the panel or using a waistbandless pouched-style carrier this does not apply).

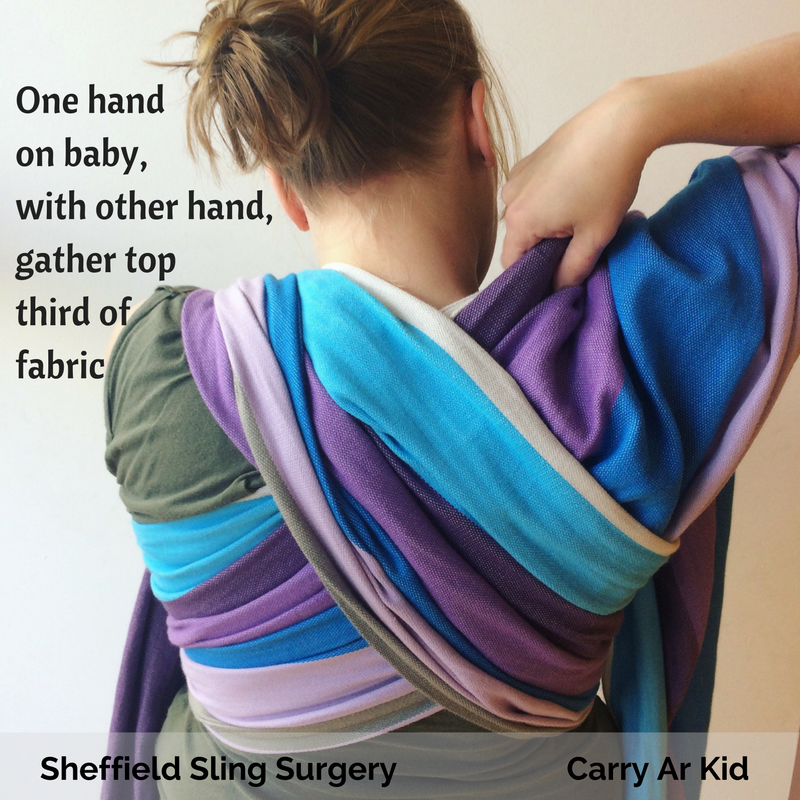
- Hold your baby in the correct position and location with one arm, resting against you, and then with the other hand, reach underneath the panel and smooth this up your baby’s back.
- If you are using an insert, make sure your baby is positioned correctly on the seat and that little feet are not being squashed but are resting on either side of the insert.
- Ensure you have a good pelvic tuck. This maneouvre encourages your child to sit in the carrier seat with their weight resting on their bottom. not in their knee pits. It encourages their spine to curve gently and will allow them to relax into you, making carrying easier.

Sort your straps
- Weight distribution is most effective when baby’s centre of gravity is closer to yours. This can be achieved by making sure your shoulder straps are snug enough to keep your baby’s chest and tummy in contact with your front, without slumping or leaning back. This will stop your shoulders and neck and from feeling pulled forwards (and prevent your lower back from having to compensate for this strain).

- Too tight straps can be uncomfortable as well; find the happy medium.
- Crossed straps that are positioned too close to the neck will be uncomfortable. Pull each strap vertically down your back and taut, before you bring it round your side to clip into the buckle. Move them further out onto your shoulder and make sure the cross is in the middle of your back before you tighten. You can use any curves that you have to help position the webbing straps and keep the cross low. Too tight straps will tend to ride up to the narrowest point.

Here is a video showing you how to fix this if you haven’t got it quite right.
- Ruck straps; the key to getting ruck straps to work is the position of the horizontal belt across the back; how high or low it sits, and the shape of the straps themselves. Too high can lead to cutting into the back of the neck, and makes the straps push up into the back of the armpits. Too low will reduce any armpit digging but can also lead to lift-off of the straps from the shoulders. Everyone has a “sweet spot” with the belt and the straps; generally somewhere in between. Get the belt right first with the help of another person, and then pull the shoulder straps snug, little bit by little bit. Pulling one side fully snug will shift the whole carrier over to the tightened side and distort the carry and be uncomfortable. This is one reason why the lift-over-the-head preclipped method of getting the carrier on can be much easier, you are not limited to a position that you can reach behind to.

Click here for a photo tutorial of this method.
Here is a video of this method.
Perfect your posture
- Many of us suffer from discomfort when carrying; much of this will be down to how we stand and how well we are aligned. Addressing your musculoskeletal health is a vital part of any carrying journey, indeed it is part of your overall wellbeing. Standing with a forward slump or rounded shoulders, or with your head hanging forward, will all distort your centre of gravity. This will mean that adding a weight to your front, however well adjusted your carrier may be, will cause strain. (image from Phi Fitness)
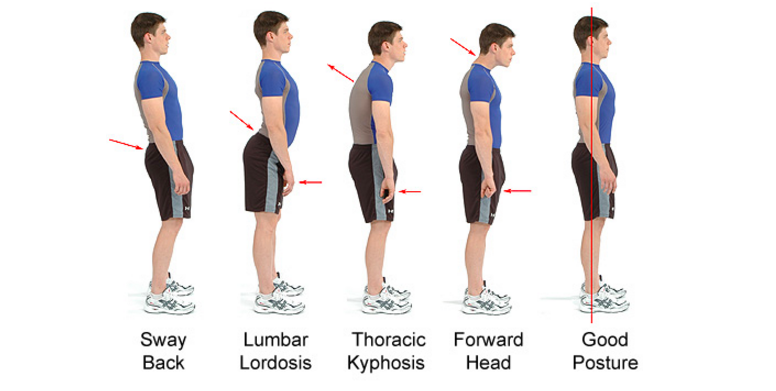
- All your major axes should be in alignment. Your head should be in line with your shoulders, and shoulders above your pelvis, which in turn is directly above your knees and ankles. It is common for people to have a pelvis that is not in neutral positioning, which significantly affects your spine and your shoulders; all our joints are connected to each other. Many of us walk with a strong forward lean due to tight calf and thigh muscles. Working on loosening these muscles to increase flexibility and adjust how we stand is very important, as is foot health.
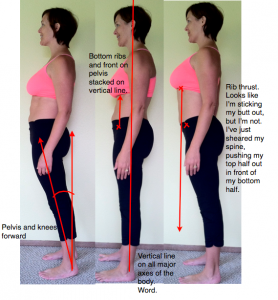
- It is worth looking at yourself side on in a mirror and watching what happens to your posture as your carrier goes on, and what it is like after ten to twenty minutes of carrying. This will help you to gradually work on how you stand as you carry and improve your comfort. (Image from Nutritious Movement/Katy Says blog)
Take your time
- Carrying loads requires a gradual build up of strength, just as training for any exercise. Muscles tone and become stronger with use. Increase the amount of time you carry your child bit by bit, massaging and winding down your muscles after any discomfort.
See your sling library for help
- you can find your local resource here www.slingpages.co.uk

Guide to Slings
A guide to slings: choosing to carry your child is just the start of an adventure you can share together and both derive a great deal of enjoyment from! It can often feel overwhelming, trying to decide what to try first when there are so many options and everyone has their own favourites. Our guide to slings is designed to help you understand the basics of safe sling use and to know more about the major types of sling.




Useful videos can be found here and the photo tutorials here.
Read more about Common Queries here (such as facing out, carrying in the post-natal period, healthy hip positioning)
Read more about Carrying in Special Circumstances here (such as carrying while pregnant, carrying older children, carrying premature babies)
Do get in touch if you need some help.

Welcome to Slings
Welcome to the wonderful world of slings! You may be new to carrying and a bit overwhelmed about the choices available. You may be just starting out with your carrier and not sure if it’s the best or most comfortable option and wonder what else there may be. Read on for more information about how to make babywearing work for you, your baby and your family.
New to slings?
Not sure where to start when it comes to using a sling? This is a common concern among parents who have become convinced of the benefits of carrying their baby but feel a bit all at sea about the huge variety of slings and the confusing jargon in the sling community.
- There are many positive effects of using a sling with a very young baby; there is much evidence to suggest that skin to skin contact between mother and newborn (especially premature) babies can confer great advantages on both. The baby gains assistance with their physiological regulation of breathing and heart rate, temperature control is improved, and the contact helps to establish breastfeeding and promote more rapid growth compared to babies who are not held as close for as long. Furthermore, the baby will feel more secure in his developing relationship with his caregiver, due to the time spent in close contact.
- The caregiver enjoys positive effects too; he/she may find themselves more able to bond with their baby, due to the increased release of oxytocin, and post-natal depression may be reduced. Being able to be “hands-free” can really make a difference to a family’s ability to get around with their new baby, keeping them active and engaging with normal life.
- There are also many positive effects for society; such as a reduced burden of mental health and greater fitness.


Firstly, make sure you choose a sling that allows you to carry safely.
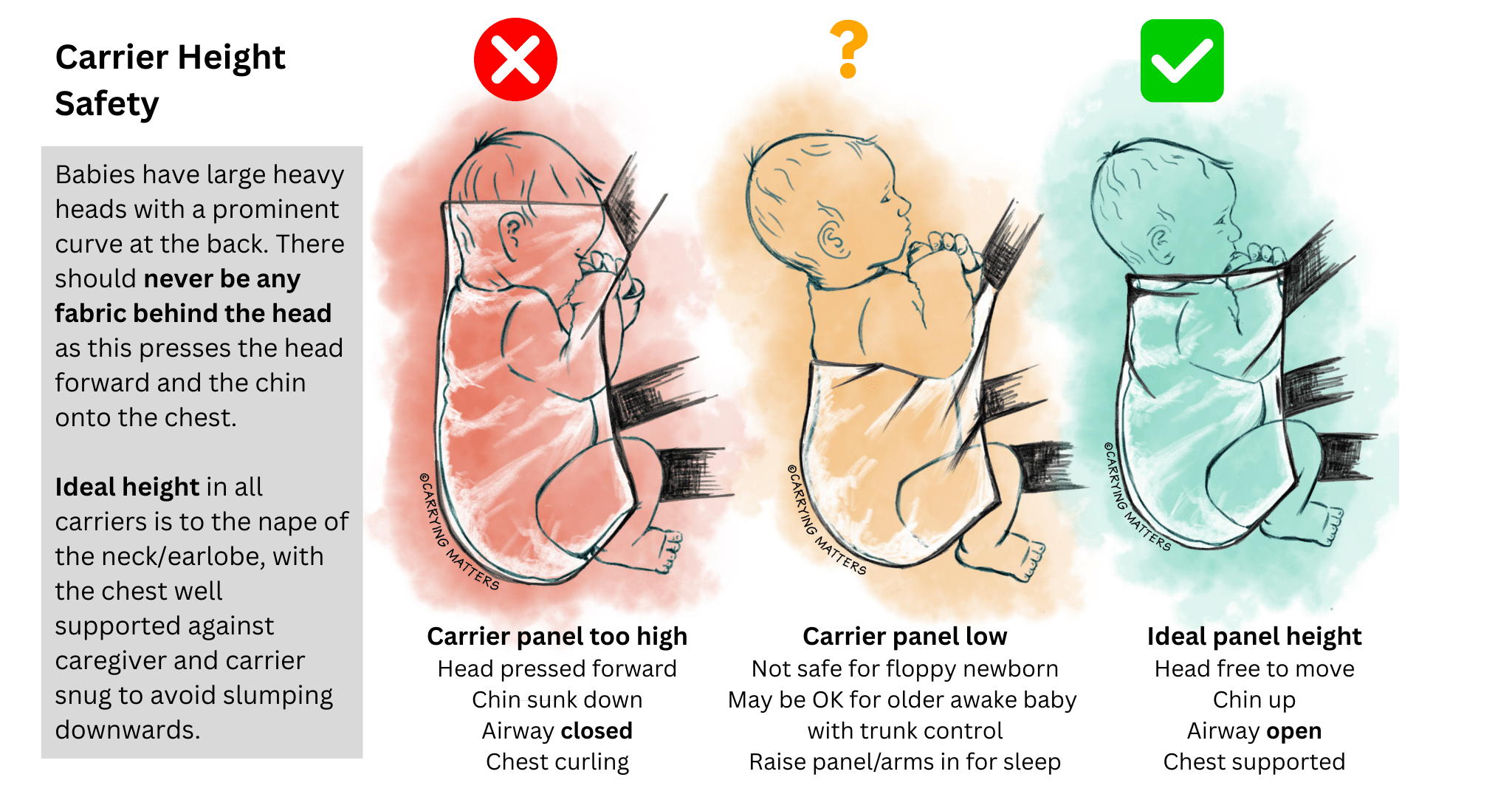
This is especially important with young babies who are still small and in need of “fourth trimester” nurturing. In summary, a baby’s airway should be supported with the head well aligned with the spine, thereby avoiding curled-up into ball positions that could impair breathing. Carriers must not be too tall, do not be tempted to tuck your baby’s head down inside a carrier for “head support”.
 The safest place for a baby is upright, facing the parent, just as they are when carried in arms. His head should be resting against his parent’s upper chest, close enough to kiss, and supported snugly all around to avoid any slumping. Babies naturally adopt a squat position with a slightly curved lower back (you can see this in action when you lay your baby down to change their nappy).
The safest place for a baby is upright, facing the parent, just as they are when carried in arms. His head should be resting against his parent’s upper chest, close enough to kiss, and supported snugly all around to avoid any slumping. Babies naturally adopt a squat position with a slightly curved lower back (you can see this in action when you lay your baby down to change their nappy).
Ergonomic slings will respect this and carry a baby in a seated position, with the knees above the bottom. By bringing knees up, babies’ hips are rotated and do not need to be spread very wide to be resting comfortably, as the image shows. Narrow-based carriers (sold by high-street shops and online) are not always unsafe, but they are often suboptimal and may not be as comfortable for a baby to rest in as one that has a wider seat and encourages the knees to be raised.
Such hip-healthy positioning also helps to stabilise a baby’s back and protects the airway, as it reduces the amount of backward head lolling and uncomfortable straightening of a baby’s curved spine.
Click the link to read more about safe positioning in a sling and click here for information about healthy hip positioning.
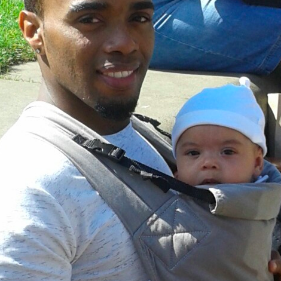
This baby has just had her stretchy wrap removed; the sling has held her in the natural "in- arms" position

Safe, anatomically correct and comfortable positioning in arms and in a carrier

Secondly, choose a sling that is comfortable
Many parents find their high-street carriers can be less comfortable than they hoped, especially as their baby grows, and may stop using a sling at all.
Good slings have been designed to mimic in-arms comfortable carrying as much as possible, and many people find they are able to enjoy long walks with their children, up to pre-school age, with such an ergonomic carrier.
Broad weight distribution across the parent’s body matters; a child who is able to snuggle in and shift their weight closer to their parent’s centre of gravity will feel a lot lighter than one who is held in a stiff pocket, or held lower down and facing out (thus pulling away from the parent).
This applies in front, hip and back carries equally. Positioning makes a great deal of difference to your child’s and your experience of the sling, and is the most important factor in how comfortable it is.
You can make your high street carrier more comfortable in a variety of ways, for example by ensuring your baby is higher up on your chest, held snugly, and using a scarf to redistribute the weight. Your baby should be held snugly enough not to swing free when you lean forwards.
Features like the type of shoulder strap (wide or narrow, those that cross over on the back versus those that are more like rucksack straps), the shape and sturdiness of the waistband, and the type of fabric used can also make a considerable difference. It is always worth trying before you buy, and there are many sling libraries around the country that can help you do this. The Sling Pages has a full list for you to check your local resources.
"Scarf hack" for narrow based carriers

Thirdly, think about what kind of sling may suit you and your family best

Stretchy Wrap
If you have a newborn or a baby under six months, most people will start with a stretchy wrap. This is usually a long piece of jersey style elastic fabric that is between 4 and 5 metres long, and can be wrapped around your body to create a snug pocket your baby can nestle into. Depending on the quality of the fabric, the stretchy wrap is usually used up to six months. It is often worth investing a little more for higher quality.
One size (usually) fits all, and it can be tied on and left on all day for convenience, popping baby in and out with ease without needing to take the sling off each time, many parents don’t realise this. It is possible to use the stretchy wrap as a breastfeeding aid, with care and attention to baby’s airway.
You can read more about stretchy wraps here, including how to use it well.
Close Caboo Carrier
This is a slightly more structured and less stretchy variant of a stretchy wrap, with a little less flexibility. It is put on, adjusted carefully, and then baby is popped into each of the cross passes on the front. The fabric can be tightened through the rings to achieve a snug fit. The Close Carrier can be used as a breastfeeding aid if required, with care and attention to baby’s airway, and most people will find it supportive up to three to four months.
Ring Slings
This is a piece of woven fabric which has one end sewn securely into two strong rings. They are worn cuppring one shoulder with the child sitting in a pouch on the opposite side of the parent’s body, with the loose end of the fabric threaded through the rings in such a way that the tension holds the fabric firmly and the weight is distributed across the shoulder and back.
They have the advantage of being lightweight and (once the knack is gained), quick to put on and take off. They can be very useful for those who need to be able to carry their child on the hip, or need something that offers the child a good viewpoint in all directions.
Ring slings made of woven fabric and with no padded rails are usually the best option, and shoulder style (pleated or gathered) is a very personal choice. They can be used from birth to toddlerhood, and it can be easy to breastfeed in a ring sling, with the appropriate attention paid to airway and positioning.
Hip carriers
Pouches are another kind of hip carrier which can be very simple, but need to be fitted to size; they can be a risk for babies under 3months if used badly.
The Scootababy is a buckled hip carrier with a waistband which can be used from approximately four months and up into toddlerhood.
Carrying aids and hip seats can make hip carrying easier but are not hands-free.
You can read more about ring slings and hip carriers here and your local sling library will be able to help too.


Woven Wraps
Woven wraps are excellent choices if you want great comfort and longevity. They can be used from birth to toddlerhood and beyond. Woven wraps are long parallelogram shaped pieces of fabric, anything from 2 to 7m long.
They are woven in a particular way to provide gentle all-around pressure, supportive but still soft and mouldable. Most woven wraps are made of cotton, some may contain other fibres such as linen or hemp, for extra support, and come in many different colours and designs.
Many women around the world use local woven cloths for many purposes as well as for child-carrying. These cloths and woven wraps feel very different from the fabrics you might find in a haberdashery shop; these are more likely to fray and tear.
Many people begin with a 4.6m wrap (known as a size 6) and learn a carry known as the Front Wrap Cross Carry. They can take a little practice but they allow a great degree of adjustability and weight distribution around the body. There are numerous ways to tie the same wrap, so they can be used on the front, hip or back at the appropriate ages. Your local sling and carrier consultant or sling library will be able to get you started!
Upright breastfeeding is possible, if done safely with the appropriate attention paid to airway protection.
You can read more about woven wraps here.




Meh Dai/Bei Dai (formerly known as Mei Tai) Carriers and variants (half buckles, onbuhimos, etc)
These are Asian inspired carriers made of soft fabric, and are popular with those who appreciate the mouldability and support of woven wraps but need something with more structure, or speed of use.
They consist of a fabric panel that has two straps at the base which are tied or buckled securely around the waist, and two straps from the top of the panel which can be wrapped around the parent and baby to ensure a snug and comfortable fit. Baby sits in the pouch created by the panel, and the long straps allow a great degree of adjustability to all shapes and sizes. They can be worn on the front, hip and back at the appropriate ages, and upright breastfeeding is often possible, if done safely with the relevant attention paid to airway protection.
Your local sling library should have a few of these to try out.
You can read more about meh dais and their variants here.
Full Buckle Carriers
If you’re not sure about tying fabric, a good option is a full buckle carrier, which has a buckle on the waistband, and the shoulder straps buckle into the panel at the sides. Baby is seated facing the parent, inside a supportive pouch that supports them widely across the base from one knee to the other.
Waistband types vary, from the minimal to the heavily padded, and people’s preferences vary enormously. Some shoulder straps cross over on the back when baby is on the front, others are fixed into a rucksack style. The shape of adult and baby together is very individual, as is the health of the adult’s back, so what suits one pairing will not suit another. More padding does not automatically mean “better” or more comfortable, and those with back pain will not always need heavily structured slings. Good posture and general back health are important – read more about this here.
Buckle carriers can be very quick and simple to use. Often, a little practice to get the straps and positioning optimally adjusted is well worth it. Most good full buckles fit well from three months upwards; some can be adapted for younger babies by rolling the panel or by using inserts to keep baby snug, high up and visible. Many carriers will last into early toddlerhood, and some beyond that, depending on design.
Many mums find that breastfeeding in the buckle carrier is possible, if done safely with the relevant attention paid to airway protection. Most can be used on the back once babies have grown.
Some buckle carriers will allow baby to face the world. This can be great, when done safely and responsively. It is recommended only from four months upwards, not for sleeping in to protect the airway, and only for short periods of time. This is due to the reduced opportunity baby has to see and interact with his parent and learn about the world based on his parent’s response to it – this is known as social referencing. There is also reduced hip and leg support from the narrow base which can be an issue in some circumstances, as well as less comfortable for child and parent. Carriers that provide hip healthy positions facing out are generally preferred. (read more about facing out here.)
You can read more about buckle carriers here.




Fifthly, enjoy your sling and let the world see it!
Why not share your enjoyment with the parents you meet so they can discover slings too? We all carry our babies, some in arms, some in high street carriers, some in wraps, some in ring slings, some in meh dais, some in buckles. We all learn from each other; encouragement is always more productive than criticism!
Here is a lovely article from Ellie at Peekaboo Slings about the importance of no judgment; “We want to normalise babywearing and promote carrying your children close – put bluntly, we don’t care about the rest”.
Fourthly, be aware of the changing needs of your baby
The weather conditions may change how you carry your baby; being aware of the heat and the sun, or the cold and the rain may affect your choice of sling and your clothing.
As your baby grows, her own needs will change. She may want to sleep less and look around more. She may prefer hip carries, or even back carries, so she can see into the world into which she is being carried. As she gets heavier, the carrier you began with may begin to feel less supportive for you and for her; for many this marks a move towards “toddler-worthy” carriers. This may be different ways of tying your woven wrap, learning how to adjust the straps on your meh dai to ensure knee to knee support, or moving up to a bigger, toddler-sized (or even preschooler!) carrier when you need to. Your “baby” sized carrier will often last a lot longer than you think.
You will not spoil your baby or make him clingy by carrying him as he grows. Big kids need cuddles too – loving contact is vital to our emotional health and security, from cradle to grave. You can read more about carrying older children here, and your local sling library or consultant should be able to help you make the most of your carrier.


How to Choose a Sling
I have met thousands of parents over the years, wanting help with choosing a sling. It’s fantastic to support them in their desire to carry their child close, with all the great things this will bring the whole family. For many, they can feel utterly overwhelmed by the huge range of options on offer (see here for a quick introduction to carrying, and here for a quick overview of the major types of sling).
Very often, they will ask me what I would recommend.. and this is a very hard question to answer, one that I usually respond to with more questions! Everyone’s choice of carrier is unique for themselves; and their initial choice will often change as they try things out.
Initially, when it comes to choosing a sling,
many people will look for a carrier that isn’t especially expensive, to see “if they get on with carrying.” Others will pick something that has been marketed by a mass-manufacturer in mainstream stores or at trade shows as being the best option available or will have picked something recommended on social media (please be aware of the fact that many of these influencers have no idea how to use a carrier well or safely), or will choose something for the specific features listed, such as the ability to carry a baby in multiple positions, or being described as “the best”. Some may have been given carriers by their friends from several years ago (often hardly used “as it just didn’t work for us”), or bagged some ultra-cheap ones on Ebay/Vinted.
This can sometimes lead to problems, as such carriers may not have been specifically designed to work with parent and child anatomy and can thus often be uncomfortable after only a short time. They may be worn too loose or baby may be too low, causing back pain from the strain of the carrying or the hunching that can ensue (as well as potentially posing an airway risk – also see here for more about carriers being too big). This can lead to a belief that that baby is too heavy or that the parent isn’t strong enough (neither is usually true!) and carrying journeys come to a premature end. At this point, those who want to make carrying work for them will often look for support from someone like me to find something that works. Of course, some parents will come straight to us right at the start!
A good carrier should be comfortable for both baby and parent. It should support baby safely, protecting their airway and allowing easy breathing, in just the same way as when you hold them upright on your chest in your arms.
A good carrier should hold baby in the anatomically appropriate spread-squat position that respects infant and child spine physiology, and it should be snug against parent/caregivers chest for weight distribution. Carrying in this fashion is safe, and is usually much more comfortable and allows longer duration of sling use than in-arms or in a poorly fitting carrier. (Do remember to build up your carrying muscles day by day. It is exercise and gets easier with repetition, just like training for a race.)
People end up choosing their main carrier for many different reasons – and each individual will have different priorities, which will lead to their own personal choice. When I am asked what I would recommend myself, I often describe a bar chart like the one below, which shows just how variable things can be, and what suits me won’t suit them. Some people will prioritise comfort and longevity over pricing and simplicity; some value customisability and appearance more than pricing or resale value, everyone is different. People may end up choosing alternative carriers that they had originally envisaged, based on their “list of requirements”, due to how the sling feels for baby and parent when it is fitted.
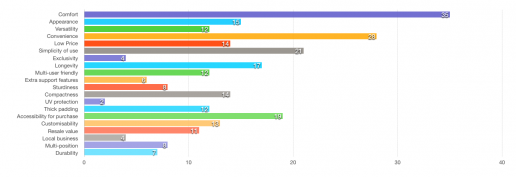
This is why one “size does not fit all” and why many of us in the sling world use an analogy of shoe fitting, jeans or wedding dresses when it comes to trying a carrier. Everyone ends up with something difference. Cheap shoes bought over the internet often don’t fit your feet and can cause blisters. Jimmy Choos, Louboutins or Doc Martens really do not work for everyone, however desirable or pretty or cool they may be. What works for your friend, or for a large number of enthusiastic sling owners on the internet, or an experienced sling professional may not work for you. Current trends or famous brands don’t equate to an instant “perfect fit” and no one carrier can claim to be “the ultimate” or “the best.”
Trying a few things out before you commit yourself to a purchase that can feel expensive is very useful, and it is often worth spending more on a good quality carrier that fits you well, to ensure you and your baby are both comfortable and that it will last for some time. Many people find, however, once they have the right sling, it gets used daily, and the cost per use per day comes down to pence. Don’t be tempted to buy an extremely cheap carrier that may well be a fake (Ergobaby is the best known carrier to have been counterfeited) – always ask for proof of purchase from an authorised retailer when buying second hand. Your child’s safety isn’t worth the risk. Buyer beware!
Once you’ve recognised the benefits of carrying as comfortably as possible, how do you begin to choose?
I highly recommend visiting your local sling library to try out several options; there will be someone there with training and experience to help you navigate the choices. Some people will have a “shopping list” of requirements for their ideal carrier, based on what they have read online or been advocated by a friend or an internet group. Of course, such recommendations can be helpful, but a one-size-fits-all approach rarely works in practice. Every baby-parent dyad is unique, with their own personal stories that influence how they stand, how they carry, how they prefer to be held, for example, and particular features that seemed desirable on paper may not feel quite right in person. If you think your other half is likely to carry too, do bring them along to try things themselves; it is very hard to guess what will work.
For example, some people will love the feel of thicker, more padded waistbands, while others will find them bulky and restrictive. Some will prefer straps that cross over, others find this can ride up to the neck. Some find rucksack style straps hard to do up. Some inserts are simple to use, others more complex, many don’t like inserts at all. Some people find meh dais and woven wraps more comfortable than carriers. It is generally a good idea to have an open mind; you may be surprised to find some things work much better than you had imagined, while others just don’t feel quite right.
Bulky carriers may not necessarily equal greater support or comfort for everyone, and too much bulk can be unhelpful for some. Knowing how to achieve good positioning and how high and tight to have a carrier are very effective tools for successfully distributing weight comfortably.
A good sling librarian or peer supporter will be able to show you how to position your child, as well as tips and tricks that can make things much easier (such as how to put on fiddly straps, or how to make sure your stretchy wrap is tight enough, or how to ensure your ring sling feels secure). Sling libraries are fantastic resources.

It is worth being aware that knowledge about sling safety and best practice positioning is improving all the time. Older carriers and older brands may have instructions that are no longer part of current safety guidelines; social media is often marketing focused and wildly inaccurate, feeding and sleeping positions in slings are often out of date. Do check with your local sling professional if you have any concerns at all, they will be only too pleased to support you and your child.
Your sling should bring you and your child great enjoyment and should not cause you pain or be uncomfortable. Furthermore, as a family’s familiarity with slings grows and as their baby gets bigger, their choices can change. They may move from things that are especially designed for small babies, or carriers that are as simple as can be, on to things that they find increasingly versatile and comfortable. Babies may wish to change how they are carried, desiring greater visibility, for example. Each parent may have different shapes too, and families may decide to have different carriers for different situations (eg a simple buckled carrier for use on a school run or on a muddy day, or a woven wrap for a long sleep-inducing walk, for example). There are no “perfect” answers, but options that end up being the best choice for the circumstances.
Sling Safety Matters - How to Use a Sling Safely
Sling safety matters. Carrying our children in a sling safely can be one of the most precious experiences we ever have as parents or caregivers. There really is something very special about the bond that builds from keeping your child close.
However fantastic it may be, it must be done safely, for your baby’s health and your own. As parents of small babies and bigger ones, one of our greatest priorities is to keep our children safe. A good, correctly fitting sling can be a very helpful tool for this; keeping a child safe while daily life continues.
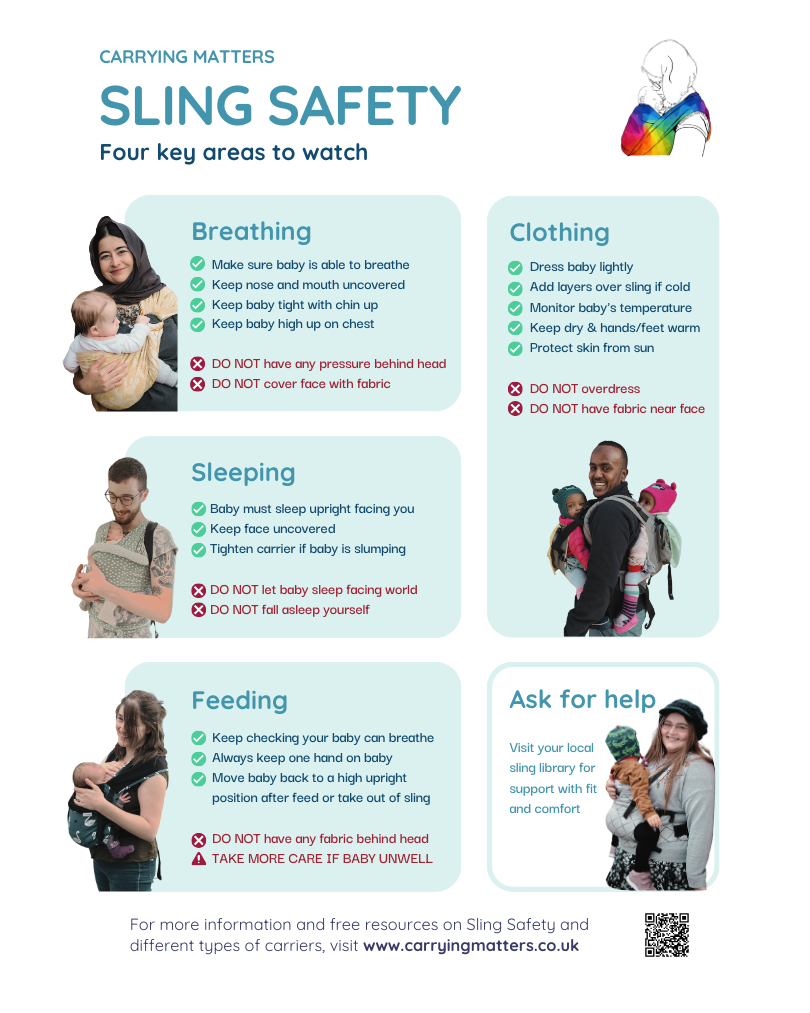
Four key areas to watch – see more detail of this image at the link here
Sling use for very young babies (birth to four months)
This is becoming increasingly popular around the more developed world; a practice that has in fact been universal for thousands of years. Families that live in extended communities or “villages” are usually able to share well-honed, tried and tested knowledge down the generations and provide easily accessible advice and support. This kind of local support is much harder to come by in our more fragmented societies, which means we often turn to books or the internet to fill the gaps in our knowledge and provide us with reassurance we are doing it right. Unfortunately, sometimes these sources of information are out-of-date, incorrect or even dangerous, and can lead to problems with the use of any kind of baby equipment. Manufacturer instructions can be slow to be updated with new “best-practice” guidelines and YouTube videos not made by professionals can often be misleading and miss out important information.
Many carriers on the market hold babies very low down and loose, which will allow young bodies with little muscle tone (especially during sleep) to slump and end up with nose and mouth pressed against fabric. This is an airway risk. They often talk about “head support” but use rigid high backed panels that tip baby’s large head and chin forwards onto their chest. This is not wise or responsible. Read more here.
 Very few manufacturers advise about monitoring baby’s temperature in baby carriers; which is important, as overheating is risky.
Very few manufacturers advise about monitoring baby’s temperature in baby carriers; which is important, as overheating is risky.
Why bother with a sling at all if there are any risks?
There are many benefits to using a sling with a very young baby; in fact. many hospitals use them in the practice known as “Kangaroo Care”, and there is much evidence to suggest this skin to skin contact between mother and newborn (especially premature babies) can confer great benefits to both.
The baby gains assistance with their physiological regulation of breathing and heart rates, temperature control is improved, and the contact helps to establish breastfeeding and promote more rapid growth compared to babies who are not held as close for as long. Furthermore, the baby will feel more secure in their developing relationship with his caregiver, due to the time spent in close contact.
The caregiver may find that he/she is able to bond with her baby, due to the increased release of oxytocin, and post-natal depression may be reduced. Being able to be “hands-free” can really make a difference to a family’s ability to get around with their new baby, keeping them active and engaging with normal life.
The key is to know how to use the sling in a safe and secure way, just as you may practise learning to ride a bicycle, or drive a car. Familiarity and practice make perfect. All baby equipment should be used safely, and it is an unfortunate fact that sometimes things are not fit for purpose, or the instructions that come with equipment are inadequate. Babies should be able to breathe easily, be at a comfortable temperature, and held in positions that are healthy and beneficial for them.


How can I ensure I am using my sling safely?
A good sling should mimic the natural, in-arms upright position for carrying babies, ensuring the caregiver can see and sense the baby at all times, and thus able to be quickly aware of and rapidly responsive to any changes.
I see a lot of parents with newborn babies wanting to learn how to use a sling, and the photos and the position diagrams here are the first thing we look at.


Babies grow in tucked positions, and after birth, they tend to maintain this gentle curve to their spines for several months due their lack of muscle tone or strength to their head and neck and upper torso. It is not till they are older that they have the strength to hold their spine in a straightened posture. It is not till they can crawl and stand and are beginning to walk that their muscles and ligaments hold the spine in the more adult S shape. While babies are young, holding them in their naturally adopted tucked positions is both comfortable for them and also more comfortable for you. If their backs are well supported, their heads do not need rigid support, do not be tempted to raise head rests or sink babies down inside panels. Babies will rapidly develop head control – here is some guidance about managing a “floppy head” without compromising airway. As they grow and begin to develop their strength and clinging ability, their needs will change.
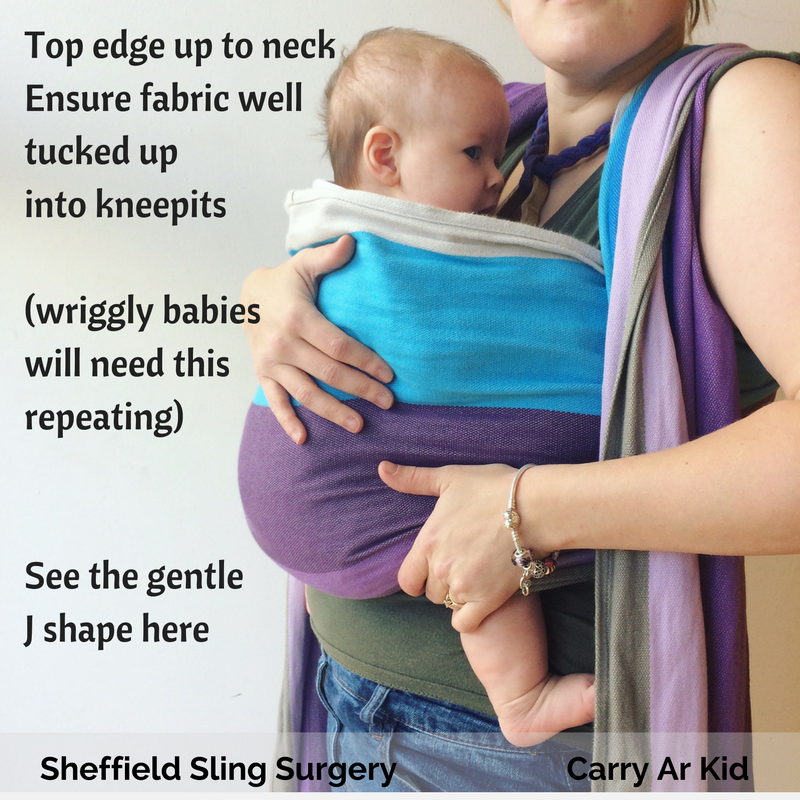
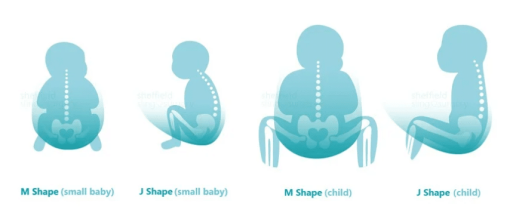
Young babies who are seated in the “squat” position or the M shape (looks like a J shape from the side) will have a broader, more stable base to rest on than a narrow perch. This position, with the curve mainly at the base also helps to keep the chest flat against the parent’s body and thus in an expanded position for good airflow.
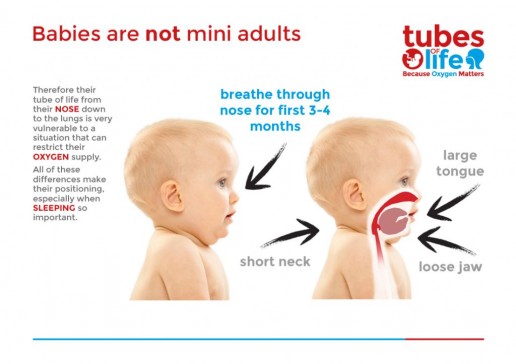

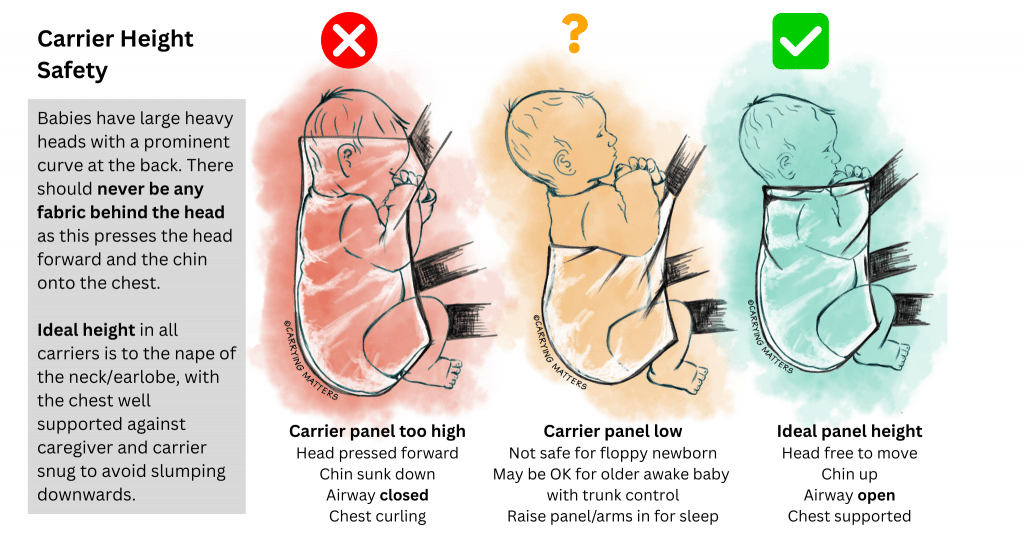
Babies under 3 to 4 months are most at risk of airway compromise when chin can sink onto their chests; so a good carrier will hold baby’s chest snugly against yours to keep the chest cavity uncurled and the chin off the chest. It is important to ensure no slumping and that there is no fabric over the face and there is a good air supply. Babies have a disproportionately large occiput (the back of the skull) and a short neck, along with lower muscle strength and co-ordination compared to adults. Rigid surfaces behind the back of their heads tend to push the skull forwards so chin sinks onto chest and can obstruct airway. This is is why upper back and neck support (no further up than the earlobes) is so important, rather than using headrests which can be risky.
Stabilising a child’s body with a broad base and good upper back and neck support is key in the early months.
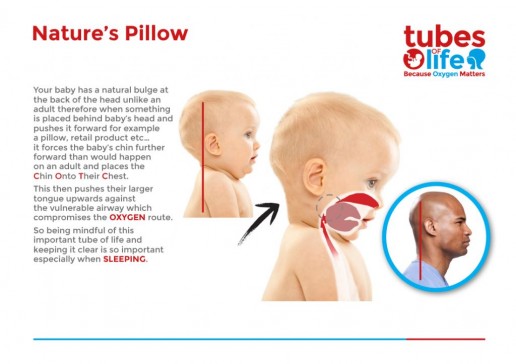
This also applies to car seat usage; rigid shells with a hard back holding babies at 40 degree angles can also push a baby’s chin onto their chest and is why it is not recommended for newborns to sleep for long periods in car seats.
Babies should be dressed appropriately to ensure they do not get too warm; people are often surprised how quickly everyone can warm up when in close contact. Please do not use thick, furry or padded snowsuits and dress down. You can always add more layers over the top.
Respectful, anatomically appropriate positioning
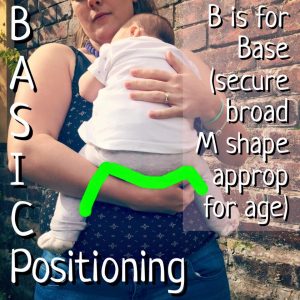
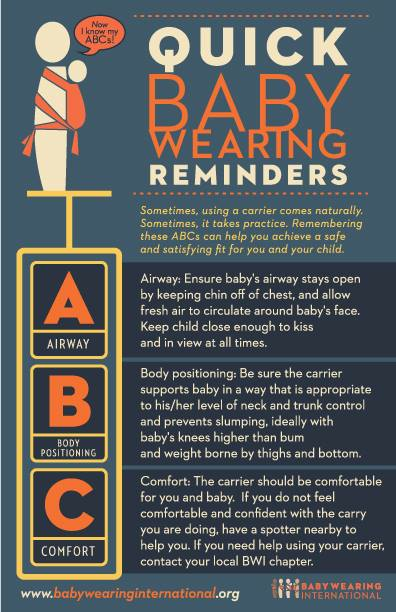
ABC is the basic first-aid mnemonic, which can be adapted for safe sling use.
AIRWAY is vital. Babies’ heads are heavy and it takes time for their muscle strength and tone to develop enough to hold up their heads and support their own airways; until then, it is our job as parents to be as caring and careful as we can. A baby’s head should be resting against the caregiver’s chest, with the windpipe straight, not curled over. A good guide is at least two fingers being able to fit between baby’s chin and his chest. Air should be able to circulate freely and the face should not be obscured by fabric, or buried within cleavage. Baby’s cheek can rest against parent’s chest, and hands should be accessible to the mouth for sucking if needed (and not trapped down the side of the sling)
BODY POSITION is important to protect the airway as well. The upper body should be supported against parent’s chest, to ensure no slumping (this is why carriers should be tight, to make sure that babies do not roll up into a ball). The pelvic tuck into the M shape with knees higher than bottom will help support baby’s back as well as being very comfortable. The neck should be supported where possible to avoid backwards lolling but the back of the head should never be tilted forwards (see the image above – babies have a larger occiput, shorter neck and less-strong neck muscles than adults). The pelvic tilt and using a rolled muslin cushion (to rest below the earlobes) can be helpful if babies resist head support. See the diagrams above for the correct shaping.
COMFORT comes last – I would rather see a child in an uncomfortable carrier that was safe, than fast asleep slumped into a tight ball or folded over in a cradle carry, however comfortable it is. However, you and your child are likely to enjoy and appreciate a carrier that is pleasant to use, fits well and does not cause back pain. Here is some advice about how to choose a carrier. Comfort also covers the baby’s temperature; too hot is a problem, so please layer your baby carefully and do not over-dress them.
In summary, the safest position is an upright one that meets the TICKS guidelines – Tight, In View, Close enough to Kiss, Keep Chin off the Chest, Supported Back.
I would never recommend any kind of lying- down position in a carrier, especially where the back of the head is bent forwards to compress the airway and a child is thus not able move its head freely to clear any blockage. Bag slings, ill-fitting pouch slings and other slings used badly can be risky.
Breastfeeding is usually safest done in upright positions for this reason, and a child who falls asleep feeding in a sling should always, always be brought back into this safe upright position, to protect the airway. Babies should never be left to sleep in a cradled position inside a sling; this can be dangerous.
What about older babies beyond the early weeks and months when they are developing more control over their bodies?
As babies grow, their needs and abilities change. A baby who can maintain their own airway independently will expect more freedom and will show you this with wriggling and turning. Their wild jerky movements are how they practice muscle control and learn coordination. Movement is important, babies should be given the opportunity to explore their bodies whenever possible. Parents and carers will need to find a happy balance between the need for safe and comfortable transportation, a place to sleep or feed, and their baby’s need to move. It’s worth being aware that prolonged, unchanged positioning isn’t good for anyone and even adults are being encouraged to move every 45 minutes. Children’s bodies are still growing!
Try to change positions, try in arms carrying, swap with other carers, use a buggy, to give children a variety of experiences and positions.
Top Tips
Position matters
- Your child must be able to breathe safely in the sling. Their chin should not be touching their chest (a good guide is a space two finger-widths or more) or lolling back too far. (Try it yourself! Can you swallow your saliva with your chin too close to your chest or lolling all the way back?)
- To ensure no slumping, position your child correctly against your body, chest well against yours, and bring the carrier over your baby as you hold them. This video will help you to ensure no slump.
- A child whose bottom and legs are well supported from knee to knee in a “spread squat” or “M position” is in a more stable position and will be less likely to fold up or slump over.
Know your sling and know your baby
- Always familiarise yourself with your carrier before you use it for the first time. Ensure you have a good idea how to use it. Some people like to practice with a teddy bear near a bed and with a mirror to see what is happening.
- Always check your carrier before use for any wear and tear, that all component parts are present and fit for purpose (eg is the chest belt in place? Are any buckles in the right places and not broken, are the seams are intact?)
- Check your baby is willing to be carried. The only “unsafe” carry is one with an unwilling baby. If baby seems unkeen, can you establish why? For example, is he hungry? Is she wet or dirty? Does he have reflux or does he find certain positions uncomfortable? Does she want to do something else? Is he too hot or cold? Is she in pain? If he or she cries in a sling, read here about some of the many other reasons a baby may express distress.
Dress appropriately
- Ensure appropriate clothing – the sling may add additional warmth, so layering is a good idea.
- In cold weather there is a temptation to wrap up extra warm but this needs to be done with care. Too-warm babies are less likely to wake if their breathing slows. Don't be tempted to over-dress!! You can always add more layers over the top if babies really are cold.
- Many people find baby leggings, gloves on strings, well fitting hats and tie-on warm booties to be especially helpful in the chill. Thin layering is key.
- Read more about the risks of snowsuits here.
- Don’t forget to ensure your baby doesn’t get too hot in the summer; protect your baby from sunburn and to keep well hydrated in warm weather.
- An useful tip, if you dress your baby in a bodysuit with feet, is to choose a larger size than for ordinary wear, as the fabric will ride up a little with the sling and may squash tiny toes.
Be alert at all times
- It is important to be aware of your child at all times; if you feel something is different, check! Some people like to carry a small pocket mirror so they can check on children riding on the back.
- It is wise to consider what physical activity you wish to do while babywearing; will it hinder your awareness of your child in the sling or hamper your ability to deal with any problems? Your baby will be at a height in the sling and may be able to reach for unexpected items – awareness and attention is vital.
- Be very cautious when engaging in any form of exercise or dance with your baby in the carrier; many manufacturers do not recommend this, and there are risks with young babies and untrained class leaders. Read more about slings and exercise here.
- Your sling is NOT a substitute for a car seat, and you should not sleep while carrying your baby.
- Do not carry your baby facing out in a carrier before 3-4months, and avoid letting them sleep facing out. Be responsive to their needs and turn them back to face you when showing signs of weariness. Choose a carrier that will be comfortable for their spines.
Get help and support
There are many, many sling communities in the UK, sling consultants like myself who offer one to one sessions where you can look through the options and practice using a carrier safely, sling libraries with trained peer supporters where you can try out slings and get some advice, and sociable sling meets that will serve a “village” purpose for parents to share their growing knowledge/personal journeys and offer support. Don’t rely on books/pamphlets/the internet – be armed with education and take advantage of the experience you will find in your local resources.
If you are unsure, do find your local sling professional at the Sling Pages – we are always happy to help.

The Fuss about Facing Out
 One of the most common “controversies” in the babywearing world is the “fuss about facing out” that is, the issue of babies being carried in facing out positions. This means babies being held with their backs to their carer, facing the world, rather than facing the person who is carrying them. Opinions vary widely among manufacturers and parents and even among professionals. Many babies do very much enjoy being held in positions where they can see the world, so why all the fuss? Is there any need for a fuss at all?
One of the most common “controversies” in the babywearing world is the “fuss about facing out” that is, the issue of babies being carried in facing out positions. This means babies being held with their backs to their carer, facing the world, rather than facing the person who is carrying them. Opinions vary widely among manufacturers and parents and even among professionals. Many babies do very much enjoy being held in positions where they can see the world, so why all the fuss? Is there any need for a fuss at all?
What are the advantages of world-facing?
Babies do enjoy seeing the world, especially once they are a little older and have mastered head control and wish to be more involved with their environment, rather than sleeping or snuggling in as they did when they were very little. Curiosity often coincides with increased motor co-ordination and greater periods of awake and interaction time. This is often the point at which families begin holding their babies in positions that give them greater visibility. Instinctively, they tend to support their little ones in very gentle positions that still ensure good hip and spine support; cradled in arms with chin off chest, or held in semi-seated positions with back curved against parent but hips held in flexion, as if sitting in a bowl.
These positions protect the natural anatomical curve of the immature spine and do not straighten it uncomfortably.
As babies grow, their muscle strength increases and fatiguability decreases, alongside greater coordination and gross motor skills. This allows slowly improving head and neck and upper back control (with less drooping or wild flailing) as their spines gradually begin to uncurl. Furthermore, as their focal length improves and visual acuity rises, the world becomes very interesting! There are stages in baby development when babies seem to arch away in arms a lot; this may be related to a desire to see more, but may also simply be attempts to hone upper back strength, in preparation for turning skills and rolling over. This is very common around ten to twelve weeks. Babies may also arch when they are tired, if they have reflux, if they are frustrated.
In-arms holding is responsive, which is the key issue; if baby makes a protesting movement or noise, the carer responds and moves the baby to help it to become calm again. Also, parental arms get tired and baby is easily moved to another position, this may often be on the shoulder facing parent again for a while. Such reactive carrying in-arms, with changing facing-in and facing-out positions, is of great benefit for honing development and also to encourage learning about the world from a safe and comfortable position.
This all sounds great, so what’s the problem with using a sling for this?
What are the hazards of facing out?
It is important to remember that young babies are not ready for prolonged and intense interaction with a very sensory-overloading environment; they have not yet learned how to process the bombardment of information their brains are receiving. They have not yet discovered how to “filter out” the irrelevant for a more focused look at the world, (a skill that we take for granted) so this can be very tiring. Being able to turn away from the noise and bustle and fall asleep (to process information) is important. Babies should NOT sleep facing out.
A facing-out carrier holds a baby in a fixed position for a prolonged period of time. The duration of this time is entirely dependent on the parent; they are unable to see their baby’s face to pick up early cues of tiredness or distress or breathing difficulties, and they are less able to feel subtle shifts in baby’s body signalling discomfort or a need to change positions. Babies can easily be left in carriers for much longer than they would be held in arms.
Babies are intensely social creatures and learn to regulate and control their emotions from interaction with their parents and watching their faces. Social referencing (also known as triangulation) is very important in the first year and well into the second. A child will often decide how to react to a new experience after it has looked to its carer; it will be less likely to touch something dangerous if the carer reacts in an upset way. Potentially scary experiences can defused by turning the head to see a parent remaining calm, or to receive comfort and reassurance, and vice versa. In a structured carrier worn facing out, it isn’t as easy for a baby to twist around to see the parent’s face for reassurance or to be able to seek comfort.
 Many pushchair makers now include parent-facing positions as standard, as this is believed to encourage and improve language skills and bonding. (It is worth noting that there is no formal evidence to suggest that our children are any slower at language acquisition than previous generations who did not use facing-out means of transport, however, anything that promotes bonding and communication is to be encouraged.)
Many pushchair makers now include parent-facing positions as standard, as this is believed to encourage and improve language skills and bonding. (It is worth noting that there is no formal evidence to suggest that our children are any slower at language acquisition than previous generations who did not use facing-out means of transport, however, anything that promotes bonding and communication is to be encouraged.)
Furthermore, the world-facing positions do not provide any safe sleeping positions (all respected manufacturers say babies must be turned around to sleep; this is often missed in the small print) as there is no head support in this carry. A heavy head that is unsupported by a parent’s chest will droop forwards, putting baby’s chest under slight compression and pressing the chin downwards, potentially compromising the airway.
This is why the majority of respected sling manufacturers suggest that babies under 4months should not be carried facing out. Before this, babies simply are not developmentally ready. Beyond this age, they should not be held in carriers facing the world for longer than twenty minutes to half an hour or so. (Some manufacturers say facing out from 3 months up, some say from 5months up). I think it depends on the child’s personal developmental stage and there should really be no rush.)
There is also the issue of hip and spine positioning in facing out positions. Most facing out in slings is done with “narrow-based” carriers, as very few high street options offer wider, more ergonomic seats that protect the gentle curve of the spine and promote healthy hip development in the world facing position. Most babies find their backs are held in straighter positions than ideal, with their legs hanging straight down from their hip sockets in this narrow shaping. While there is no formal evidence that choosing a narrow-based carrier will cause any harm to a baby who has healthy hips with normal sockets, there is a small percentage of babies who do have developmental hip dysplasia that are missed at their routine checks. These babies will benefit enormously from the ergonomic seated M shape position that allows their joints to be held in the optimum angles for healthy blood vessel growth and nutrient provision, and often this positioning is all that is needed to correct mild cases of hip dysplasia. It is worth weighing up the risks and may be better to choose a carrier that holds a baby more optimally if you decide to face baby out. Additionally, it is more comfortable for a person to be seated on a broad based hammock shaped chair rather than perched astride a narrow padded beam, and babies are no different.

Carrying a baby who is sitting high up against the carer’s body with the centres of gravity closely aligned is much more comfortable than carrying one who is low down, far away, and suspended from the carer’s shoulders. The parent’s body does not form part of the support structure of the carry when facing out, so much of the work of carrying has to be done by the upper body, rather than the core postural muscles. Centres of gravity diverge further when held facing out in narrow based carriers. Put simply, carrying facing out in this style of carrier is often uncomfortable.
Ok, so what can I use to carry my curious child optimally?
It is common among parents who are considering using a sling to look for options that offer world-facing positions. This position is what is often seen in the media and is widely advertised; it may be more pleasing to see happy babies looking directly at the camera rather than away from it, which can be better for marketing purposes. As it is so visible, it becomes the “norm” and carriers that offer this option are often perceived as “better.”

Many parents believe that babies need to be given the opportunity to face the world as much as possible for the stimulation, rather than looking at their parent all the time. Sometimes this belief can be be a marker for low self-esteem in a parent; that they just aren’t interesting enough, when in fact, for many well-attached babies, their parent is their most beloved sight. This is especially true if parent and baby are attuned and the parent is responsive and communicative and able to engage happily in play with their baby. Babies are often able to pick up on unhappy or uneasy feelings in parents and can be reflexively resistant to close contact, creating a negative spiral. Lots of in-arms carrying, skin to skin, and just time spent together can be very helpful with this.
Sometimes babies may begin to resist being carried in their parent-facing positions – they may have come to associate the sling with sleeping which they don’t want to do, and they may want to be able to see more.

To achieve a good view while the child remains parent-facing, and ensure access to the world, try carriers with broadly angled straps that don’t get too close to the face can be very useful, or ones that can be tied carefully for good visibility. As children grow in co-ordination, they need less head support and often enjoy having their arms out of carriers (with the panel reaching up to the armpits for safety and support.) It is surprising how far a child can turn round to see when they can move their shoulders!  Hip carriers and ring slings will hold a child “off-centre” or laterally on the hip, for a great vantage point, and they will still be able to turn towards their parent for conversation or rest. Back carrying can be another very useful way for a curious child to see the world coming towards them. Most structured carrier makers will suggest sitting-up age to be the most appropriate time to begin to think of this option, and it is not hard to do on your own. Your local sling library or consultant (www.slingpages.co.uk) will be able to help you learn.
Hip carriers and ring slings will hold a child “off-centre” or laterally on the hip, for a great vantage point, and they will still be able to turn towards their parent for conversation or rest. Back carrying can be another very useful way for a curious child to see the world coming towards them. Most structured carrier makers will suggest sitting-up age to be the most appropriate time to begin to think of this option, and it is not hard to do on your own. Your local sling library or consultant (www.slingpages.co.uk) will be able to help you learn.
If you have a baby who is developmentally ready for facing out in a carrier and has stable hips, then I think it is just fine to give it a go! Your local sling library will be able to show you some options and talk you through which may be the most comfortable for you. Trying the carrier out first for a period of time at home is very useful to see if it really does work for you before you buy; advice from the internet is no substitute for real life trials.This period of “fussiness” doesn’t usually last long, as babies grow in co-ordination they are happier and many babies who once resisted facing in are very content a few months later in a carrier that is more comfortable with greater longevity.
In summary, facing out can be a great deal of fun for parent and child, if done sensitively and thoughtfully, with consideration to the child’s anatomical development and comfort; look for those carriers that take your baby’s comfort as seriously as yours. Try to pick a carrier that will hold baby optimally for most of the time, some come with specially designed bucket seats and others will widen for facing in and back carrying.
Age-appropriate facing out for those who enjoy it is great, when done safely! Your local sling library can be found at www.slingpages.co.uk.




Beyond the "Knee to Knee"
How much does it really matter to have a carrier that fits from one kneepit to the other? Read on for a discussion of this topic that moves beyond the knee to knee.
Quite a few people visit my sling library on the lookout for toddler carriers, as their little ones are “no longer knee to knee” in the sling that they have, and asking me what comes next!
have, and asking me what comes next!
In Sheffield the problem arises particularly in relation to Sleepy Nico baby carriers, which are very well loved here. People are reluctant to move into other carriers that may not feel so comfy,, but don’t wish to hurt their children or be unsafe by using a sling that may be too small, or moving to a “toddler size” that may actually be too big!. There is a lot of conflicting information on the internet about the sizing of carriers which many people find very confusing to navigate….
SO…
1) What is knee to knee?
Knee to knee simply means that the carrier you are using supports your child across the full width of both thighs, from one knee to the other, reaching into the knee pit. This ensures a comfortable seat for your child, more like sitting in a hammock, than perching on a stool. The diagram below shows a carrier that is reaching knee to knee, and the side on view shows how this will create a comfortable seat.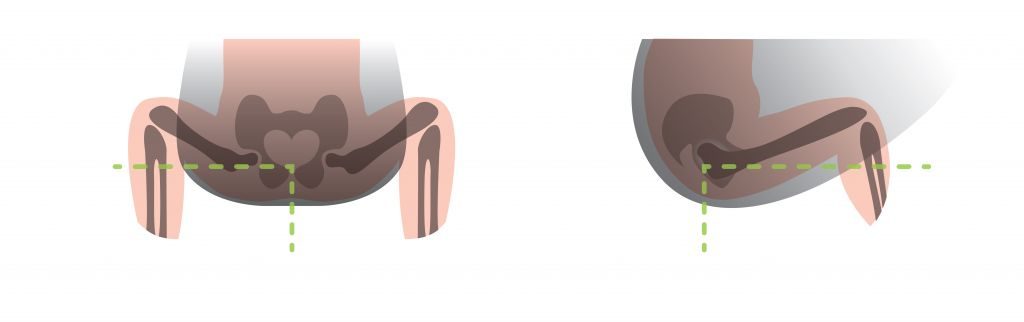
Having the knees raised above bottom also increases flexibility at the hip joint and makes it easier to flex and extend. Try it yourself! Sit astride a chair, facing the back. See how easy it is to shuffle forwards, keeping your legs flat on the chair seat, to get your symphysis pubis (the front pelvic bone) to touch the back of the chair. Those of us with lovely flexible hips who can do the Buddha position easily will find this a doddle, but others of us will find it a little sore as the ligaments get strained. You can release this tension instantly by bringing your knees up above the level of your bottom, and this will often tuck your pelvis inwards, bringing a little curve to the base of your spine. This position you have created is called the M shape, for obvious reasons, and is the ideal position, supported knee to knee with bottom a little lower. There are a few circumstances where this standard recommendation may not be appropriate, and more care will need to be taken, such as children with hyperextension conditions, or achondroplasia for a start. If you are at all unsure, do see your local sling and carrier consultant or ask for advice from trained professionals. We are always happy to help with tailored advice! For more information if a narrow based carrier will harm your child’s hips, see my “Healthy Hips” article.
2) What if my carrier seems to be no longer knee to knee?
There are usually several factors to consider here, depending on the age of your child.
Firstly, is your young child sitting in the M shape, with their bottom sitting deeply in the panel, and knees raised up with pelvis tilted? This often makes a big difference to how young children sit in carriers, and you may find it instantly makes things more comfortable for you and your child, especially if the panel has also previously felt too short. It is worth taking your time over positioning your child really well and may extend the life of your carrier for some time.
Older children who can stand and walk do not need the same level of support and will be fine if the carrier offers them good thigh support. It should keep them in a comfy seated position with lower legs bent at the knee, at right angles is fine. Older children have more muscle strength and co-ordination, and can help to grip on, so they do not need full knee to knee. They need more space and freedom to move, and will want to get down more often anyway! In this photo the sling is not reaching to the kneepit but to mid-thigh. Just make sure there is no digging in of the fabric along the thigh, and no pinning of knees with wrap fabric passes.
Secondly, is your child central in the carrier? I find that people have a tendency to hold their children slightly off centre when in arms, and then bring the panel up from that place so the child remains in a similar off-centre position. This will mean that one leg is less well supported than the other, and can lead to leaning and discomfort. Keeping a child central will often improve comfort both for your child, and for you.
Thirdly, is your child comfortable or not? Older children may be able to tell you, but for younger ones, our role as parent is to be caring and careful, and aware of non-verbal communication. Sling users usually worry (in the early stages with small babies) about over-spreading hips, as babies cry when they are uncomfortable, and children vary in their hip flexibility. This is why many carriers are “cinched” in when they are too big. Always listen to your child. If they are comfortable, and happily able to move their legs at the knee, and legs do not seem to be dragging down but are well supported, you may not need to size up just yet.
Fourthly, is your child growing taller as well? This may be more of a problem than the width of a sling if a child has a very long body and is able lean back too far from a panel that is too short. If your child leans back too far they may unbalance you. Keeping yourself and your child safe is more important than being knee to knee.
If your child is happy in their current carrier, that is good news. If they are not, and legs seem to be dangling unsupported in more of an A shape, or they are able to lean back, it may be time to consider another, bigger carrier. It might help to look in the mirror to assess your child’s leg position and how much back support they have.
3) Is it unsafe to use a carrier that is too small?
It depends on the child, and the parent! As I have pointed out in my Healthy Hips article, there is little evidence that a “narrow” seat will be harmful to any child beyond the age of six months, and even before then, the risk is low. So an older child, especially when they can bear their own weight on their legs, is not at risk of damage from not being perfectly knee to knee. They may not be as comfy as they could be if the carrier is very small and they end up with legs dangling in an A shape (this could be tiring for a child, and lead to red marks on the inside of the thighs). Let your child be your guide. I usually suggest that a carrier that supports at least to mid-thigh and allows a comfy seat with knees at right angles or a little less for older children, is fine to use.
Many big brand carriers such as Beco, Boba, Ergo and Manduca to name just a few, say that their carriers are safe to use well into toddlerhood, long after some people would feel their babies were too big for them (they are all formally safety tested). Sometimes it can seem that people are in a hurry to move out of a “standard” size carrier, before it is really necessary. Again, check your positioning, and do get some help from your local sling consultant/peer supporter/library/sling meet if you are unsure. One size does not fit all, some babies are big, some toddlers are small, some parents find bigger carriers more comfy for them, some parents find smaller carriers work better for their frames. Each carrier has its own specifications too. Some are narrow, some are short-panelled, some are wide, some are tall, some have buckles that insert very low and can squash baby thighs, etc. It is all dependent on the individual situation, and what works for one baby and parent may not work for another. Skill levels vary too, as does child compliance – a contented baby may be happy for the parent to take the time to maximise positioning, others may resist.

If you have a half buckle, or a meh dai, there are ways to tie the shoulder straps to come beneath the child’s knee, to further extend the width of the support offered by the panel itself.
4) Is it unsafe to use a carrier that is too large?
This is a more complex issue. The crucial issue to consider is child safety, based on the ABC and the TICKS guidelines. A child should not be invisible inside a carrier that is too tall, as this could be a risk to their airway and their breathing. This is one reason why many carriers have inserts, to raise children higher up the panel so their faces are visible at all times and chin can be kept off chest. I would rather see a child that was in a carrier slightly too short in the body, than in one that has too tall a panel.
As for the width and knee to knee…
A carrier that is too wide will make a child’s legs stick out straight, or he will strain against the fabric to bend his knee (which may lead to red marks, even if no voiced complaint at the time). He may feel some strain at his inner thigh if he cannot bend his knee in this hip-extended position (see the chair illustration above). Sometimes it can be suggested that the panel could be “cinched in” with something like a webbing belt, or a ribbon, etc and this may, if there is no alternative, make the carrier much more comfy as he is now able to bend his knee in the M shape. However, this will invalidate the warranty of the carrier and place strain at the waistband.
Also, by bringing the knees up higher, the angle that the hips need to open at the groin is reduced, as the joint is able to rotate more easily. *Please note that this is a hack that is rarely recommended ; if it is not in the instructions it will invalidate any warranty.*
Summary
Every parent, child and carrier combination is individual, and needs assessing as such. Many carriers that are not knee to knee may well be able to be used for your child for longer than you might expect, so there may not need to be a great rush to size up. Buying new carriers for many is great fun – if you are going to buy something too big for your child to grow into, do ensure it is comfortable for them, and not too tall. You may have more time in your current carrier than you think, to give you time to find the next carrier (if needed).
But what about the Superman Sleepy Nico at the start? Is it OK? I think we can all agree that the little SuperBaby will be OK to enjoy his special carrier for a while longer yet.
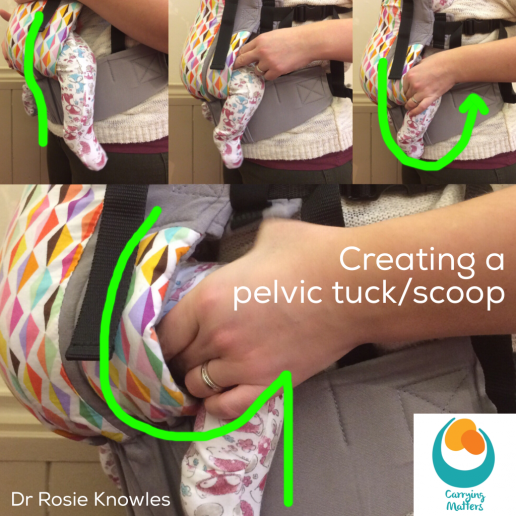
The Pelvic Tuck
What is the pelvic tuck or scoop?
I am often asked by carers who want to carry their children safely and comfortably “what is a pelvic tuck and how do I do it?”
Babies are born with gently curved spines, and usually prefer to rest in this tucked posture when they are relaxed. Arching the spine and “starfishing” can (for some) be an attempt to communicate discomfort or distress. Sleeping and relaxed babies can usually be found with their knees drawn up into a comfortable “M shape”; this is normal behaviour, and it is how most babies rest on their parents, perching on the broad secure base of the carer’s forearm. From this broad base, babies’ chests can be properly supported against the parent’s body, thereby avoiding slumping over and restricting airways.
This “squat” positioning also helps to encourage healthy hip development. Studies have shown that the rates of hip dysplasia are lower in communities that carry children on the hip or back frequently, as the posture adopted for this promotes optimum growth of the hip joint. (see here for more information on hip dysplasia and slings).
The pelvic tuck/scoop technique of encouraging a child to sit in a position that creates a “J shape” (from the side) or an “M shape” (from the front) in a carrier is therefore very helpful. Such positioning is more comfortable, more respectful of anatomy, and also helps preserve open airways. The aim is to raise the knees up, allowing the bottom to settle downwards into the classic “M shape”.

When demonstrating, I suggest that carers imagine they are scooping two curls of ice-cream towards themselves with both hands; and then repeat this action as they hold their child’s thighs gently between thumb and fingers. Another way of thinking about it is to imagine they are holding two glasses of water in front of themselves, and then pour the water out away from them.
This rotates baby’s femoral head in the socket. The photos and videos below show this in action.
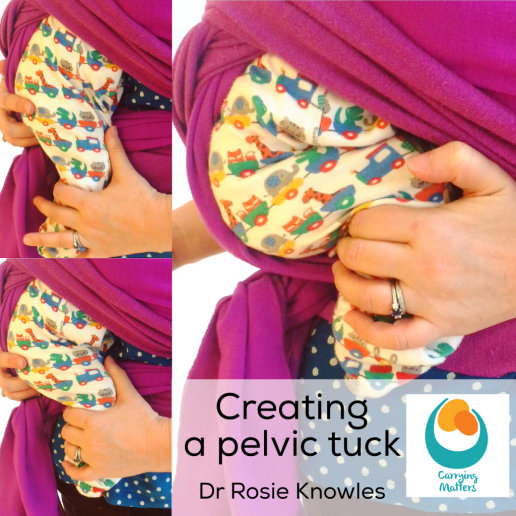
Creating this broader base seat for a younger child will also help to make a narrow base carrier more comfy and feel more stable and supportive. A simple scarf can be used to support the legs in this “M shape” once the pelvis has been tilted and knees raised above bottom.

The pelvic tuck is less important for older babies and toddlers; as children get older, the ability to actively move around in the sling becomes more important while they are awake. The key thing is to ensure they are comfortable and their legs are not dragging down or tiring them; the carrier no longer needs to be knee to knee for older children.