


Carrying in Special Circumstances
Sometimes there is a need for extra support with using slings; don’t be discouraged if you or your child have extra needs, there are always ways to keep carrying in special circumstances.
If your child can be held and carried in arms, there is likely to be a way to carry them safely in a sling. Twins can be carried in slings, as can a baby and a toddler at the same time (tandem carrying). There are ways to carry safely in pregnancy, to carry after birth, to carry premature babies. We will help you to carry your child if you have a disability, or if your child has special needs or physical health concerns. We are here to help you find a way to keep them close.
This page links to some useful information; personal stories about carrying in special circumstances, professional advice and useful links. Please see our Common Queries page for simpler situations.
If you have a special story, please get in touch to share them with me for the wider community!
I also recommend the Tania Talks blog posts on babywearing (she is a wheelchair user)
https://www.whentaniatalks.com/the-realities-of-back-carrying-as-a-wheelchair-user/
https://www.whentaniatalks.com/back-carrying-as-a-wheelchair-user/

















Here is an excellent downloadable article on Potential Therapeutic Benefits of Babywearing by Robyn Reynolds-Miller.
You can find more educational resources here for downloading (such as infographics and leaflets and images)
If you need more specialised support or have a query not covered here, please do get in touch with me or find your local sling library at Sling Pages.

Carrying a Premature Baby, personal story
This is Kay and Alex's story of carrying a premature baby. She tells us about their lives together and what role slings have played in their rocky journey. It is a truly inspiring story of great courage and endurance and I am honoured to have played a small part.
"For as long as I can remember I have wanted to be a mum, but my real journey to parenthood started 5 years ago. I decided that I didn't want to wait for the "right person" to come along and started looking into fertility treatment for single women. Unfortunately the process wasn't was easy as I expected; after lots of tests and surgery I discovered that I had endometriosis which may affect fertility..
I started out doing IVI with donor sperm but after two attempts with no success it was suggested that IVF might have a better chance of working. I decided to take part in the egg-sharing programme to reduce the cost and hopefully help someone else too. During this time there was a lot of compulsory counselling to ensure I was aware of all potential outcomes. I'm very lucky that I have a fantastic support system of family and friends around me, especially my parents.
The first attempt at IVF was not straightforwards, I got 14 eggs, (7 of which were donated), but only one was fertilised. This was put back and I got a chemical pregnancy but miscarried. I also got a relatively rare condition called Ovarian Hyperstimulation Syndrome (OHSS) which made me really ill and I had to be hospitalised on numerous occasions. Due to the poor fertilisation rate it was thought that I had poor egg quality so had to pay the full cost of IVF treatment (as a single woman I was not entitled to any NHS treatment.)
On the second IVF attempt, medications were reduced to try lessening the risk of OHSS but because doctors were anxious about this, the egg collection was done too early and 5 eggs were lost during retrieval. This attempt was unsuccessful. I again got OHSS but much milder this time. The emotional rollercoaster or IVF is unimaginable and the hormones of treatment don't help! You spend all your time so focused on preparing to become pregnant, trying to stay positive, eat well etc, then once the embryo is implanted you have the longest two weeks praying you are pregnant and counting down to the day you can take a pregnancy test... but as soon as it is test day comes you don't want to do the test because you are until then "Pregnant till Proven Otherwise" ( PUPO). Internet support groups become your sanctuary because others undergoing IVF can understand what you are feeling, while your family and friends sometimes don't understand why you put yourself through so much. IVF became my only focus.
After the second attempt I had an eight month break to save up as I had used all my savings. I decided that the next would be my last attempt and I would do everything I could to try to help it work so I would have no regrets. I changed my diet (cutting out all processed food), saw a nutritionist, had regular massage (including Mayan abdominal massage) and acupuncture. We changed the IVF regime to one that had a higher chance of success but also a higher risk of OHSS. It was a risk I was willing to take. I had partly given up hope of this round working, as I got two fertilised eggs out of 19 when I began getting the OHSS symptoms again on day 2.
I did a home pregnancy test two days before test day..... and it was positive!
I didn't know how to react, so burst into tears before laughing maniacally then calling my best friend and my parents. The excitement wore off quickly though when I was admitted to hospital with OHSS at just 4+1 weeks. At a point when I had hoped that the hard part was over, it turned out that this was just the beginning of another difficult journey.
 At 18 weeks pregnant, I began getting tightenings. As a midwife, I knew that Braxton Hicks could start early, so I just assumed it was this. though I also worried it might be something more. At 19+4 with continued tightenings, I was seen by my consultant for review and thankfully everything looked ok and possibly just a urine infection causing all this. I was reassured two days later when I had my anatomical scan and everything looked good with a healthy active baby.
At 18 weeks pregnant, I began getting tightenings. As a midwife, I knew that Braxton Hicks could start early, so I just assumed it was this. though I also worried it might be something more. At 19+4 with continued tightenings, I was seen by my consultant for review and thankfully everything looked ok and possibly just a urine infection causing all this. I was reassured two days later when I had my anatomical scan and everything looked good with a healthy active baby.
I continued to have tightenings but tried to ignore them as everything else seemed OK. Then exactly two weeks later after my scan at 21+6, I started with the smallest amount of bleeding. Again I was reassured as baby seemed OK and it had settled, possibly caused by a cervical erosion, and just to observe. I continued spotting on and off but nothing major, until I was at work on a shift on labour ward at 23+1 weeks pregnant.
I had a significant bleed and was terrified. I felt it was too far on in the pregnancy to lose the baby now but it was far too early to be born. I burst into tears. I am so grateful that I was at work surrounded by fantastic colleagues. I was admitted to the antenatal ward for observation overnight and I didn't go home again.
I continued to have tightenings and bleeding to varying degrees over the next three weeks. Getting to 24 weeks was a major milestone and I was given steroids to mature the baby's lungs. At around 25 weeks my waters went though because of the bleeding it wasn't obvious. Baby was breech and because of the situation I kept being told I might be taken for a Caesarean if bleeding increased or I went into labour. I saw paediatricians who told me stark statistics about survival rates and disability. As a midwife I knew these things but as a mum it just didn't sink in. I was tearful and losing hope. At 25+5 I had a major bleed that got me taken to labour ward and starved in case it continued and and I needed theatre. I spent the next two days in high dependency being observed and in denial.
Writing it down now it seems so silly but even given the bleeding, tightenings and water break it still never clicked to anyone that the pain I was in could be labour. At exactly 26 weeks I was found to be 7cm dilated. Two hours later I had a vaginal breech delivery complicated by the head getting stuck.
Alexander Benjamin was born weighing 1lb 12 oz and in a very poor condition.

The room was full of people but no-one was saying a word. Looking back at his notes now it says it took 18minutes to stabilise him before taking him to intensive care but it didn't feel that long to me. It seems awful to think about it now but at that point once Alex was born all I felt was relief. I was glad the pregnancy was finally over after months of feeling ill and stressed. I had spent the last few weeks trying to detach from the pregnancy as I feared the worst, but in the moment when Alex was taken away and we (myself, my parents and my friend) were left alone the silence said it all.
 I know it can often take up to an hour to get a baby settled into neonatal unit with all the lines, Xrays etc so we patiently waited. After nearly two hours I went to ask if we could see him.. the midwife came back saying the consultant wanted to come and talk to us first. I know the language of medical professionals and I honestly thought we had lost him. The consultant came round and told us that "Alex is a very sick little boy" and that the first 24hours would be critical. I think the adrenaline stopped me from feeling the full effects of the situation but looking back now at pictures and videos of those first hours has me choked up. Alex was beautiful to me, but so frail. You can count every rib and due to the manipulation of delivery his leg is almost black with bruising. He was covered with monitoring leads and various IV lines plus on a ventilator to keep him alive. He was put under phototherapy immediately.
I know it can often take up to an hour to get a baby settled into neonatal unit with all the lines, Xrays etc so we patiently waited. After nearly two hours I went to ask if we could see him.. the midwife came back saying the consultant wanted to come and talk to us first. I know the language of medical professionals and I honestly thought we had lost him. The consultant came round and told us that "Alex is a very sick little boy" and that the first 24hours would be critical. I think the adrenaline stopped me from feeling the full effects of the situation but looking back now at pictures and videos of those first hours has me choked up. Alex was beautiful to me, but so frail. You can count every rib and due to the manipulation of delivery his leg is almost black with bruising. He was covered with monitoring leads and various IV lines plus on a ventilator to keep him alive. He was put under phototherapy immediately.
Only I was allowed to touch him but couldn't hold him yet.
 My first hold came on November 17th, aptly, World Prematurity Day. I was nervous about pulling a line or hurting him but also so excited to hold him! He was put skin to skin down my top and his ventilator tubes taped to me to keep him safe. I can still smell him now and it brings me to tears. As a parent you take for granted the milestones you will see; the birth experience you imagined, the crying baby just born and put skin to skin at once. I didn't get these, and my milestones with Alex are different, but even more amazing after the challenges he has faced. We spent 135 days in the neonatal unit and I was there 12 hours a day for 133 of those days. (Two days I was ill from sheer exhaustion and wasn't allowed in.)
My first hold came on November 17th, aptly, World Prematurity Day. I was nervous about pulling a line or hurting him but also so excited to hold him! He was put skin to skin down my top and his ventilator tubes taped to me to keep him safe. I can still smell him now and it brings me to tears. As a parent you take for granted the milestones you will see; the birth experience you imagined, the crying baby just born and put skin to skin at once. I didn't get these, and my milestones with Alex are different, but even more amazing after the challenges he has faced. We spent 135 days in the neonatal unit and I was there 12 hours a day for 133 of those days. (Two days I was ill from sheer exhaustion and wasn't allowed in.)
 I spent my time holding Alex as much as I could and when he was too poorly to be held I touched him through the incubator and spoke and sang to him. I felt being physically close would help us both bond better, especially after an awful pregnancy and so much separation. I was already aware of the Sheffield Sling Surgery due to friends attending and had contacted Rosie early on in pregnancy as I had planned to carry my baby in a sling. Once Alex was over the first big hurdle of coming off the ventilator at a month old, I got back in touch to find out if slings could help us while still in the NICU. The physiotherapist on the unit was very in favour of using slings and gave me a Vija top to try, but I felt it was more comfy just using my strappy top as we got so tangled with the wires.By the time we moved to HDU it was a slightly more relaxed environment with staff that seemed more in favour of breastfeeding and skin to skin. I decided, after discussion with Rosie, to buy my first sling, a Hana stretchy wrap.
I spent my time holding Alex as much as I could and when he was too poorly to be held I touched him through the incubator and spoke and sang to him. I felt being physically close would help us both bond better, especially after an awful pregnancy and so much separation. I was already aware of the Sheffield Sling Surgery due to friends attending and had contacted Rosie early on in pregnancy as I had planned to carry my baby in a sling. Once Alex was over the first big hurdle of coming off the ventilator at a month old, I got back in touch to find out if slings could help us while still in the NICU. The physiotherapist on the unit was very in favour of using slings and gave me a Vija top to try, but I felt it was more comfy just using my strappy top as we got so tangled with the wires.By the time we moved to HDU it was a slightly more relaxed environment with staff that seemed more in favour of breastfeeding and skin to skin. I decided, after discussion with Rosie, to buy my first sling, a Hana stretchy wrap.
It felt complicated at first getting used to the technique of wrapping and because of all the monitoring it would often take someone else to help me get all the wires sorted, but once Alex was put into the sling he fell straight to sleep. I noticed that often his heart rate and oxygen sats would improve too and it made me even more determined to keep him close.

Our journey through special care gives me mixed emotions. On the one hand I would never wish this experience on anyone. The constant stress, not just for myself but also family and friends around me. The fear that if I leave, something might happen. Every time the phone rang panic would set in and don't even get me started on the paediatricians coming up to the ward!
However, my life has changed completely in so many good ways. I have realised and experienced how fantastic the care is from my colleagues. I have become closer to my family and friends and I love watching my parents with Alex. I feel I will be an even more sympathetic and understanding midwife and I hope my practice will change to support women who go through similar experiences. Most of all I have realised my dream of becoming a mum and to the most incredible little fighter I have ever met.

I feel I have a strong bond with Alex and many people have commented on how well I can read him. I believe it is because of staying close to him as much as I have and having him in the sling has facilitated this.
Alex has Chronic Lung Disease and came home on oxygen in March. He is doing incredibly well on the lowest level now, but transporting the oxygen has been a bit of a challenge for me. The canister is heavy and the container rucksack has narrow shoulders so has hurt my shoulders; trying to balance that weight against Alex has not been easy. At times I have felt isolated simply because of that. However I have met some wonderful people on my journey through special care and in the sling community (often the two groups mix!) and we wouldn't be where we are now without these challenges.
We are still using our Hana wrap, and I've been trying out a snuggly Sleepy Nico! I've learned how to use woven wraps; we are beginning to back carry; the end of the oxygen is in sight! Time to tuck Alex up into the Sleepy Nico and reconnect after a long day.


Positive Effects of Carrying for Society
The positive effects of carrying for society are many; making a change at an individual level can have a significant impact when lots of people do it! In-arms carrying and using slings is one way that we can change the future that we all have to live in.
Possibly one of the most important positive outcomes for carrying for a parent and the society we live in is the effect it can have on mental health, which is a society-wide issue.
Western society is increasingly fractured and isolated, with a decreased sense of local community and shared care. The burden of mental unwellness in our society is growing, and becoming a parent with this background can be very tough indeed.
The birth of a baby is often an overwhelming time for both parents, especially when also faced with the expectations and demands of a fast-paced culture that often judges people by their apparent productivity and appearance. It is no wonder that postnatal depression is on the rise – affecting at least 10-15% of new mothers. This is likely an underestimate as parents feel ashamed to admit their feelings, with the effects of hiding their struggle having significant knock-ons for the whole family.
Fathers are often unrecognised to have the condition themselves, and this all adds to an increased risk of children coming to harm. This is a terrible indictment on our culture and its lack of care for some of the most vulnerable individuals in our communities.
The way we live now isn’t going to change overnight; funding for parental leave or greater support for mental health isn’t going to become suddenly available, and the media bombardment of products for parenting won’t vanish. But neither are the emotional needs of young children going to go away, especially if we want them to grow up well and be happy, confident mature individuals who are well integrated into society.
We need to find ways to nurture our children while still functioning as our culture expects us to, and this is where carrying children (often using a sling) can help. Carrying children encourages and protecting parent’s precious closeness with small children while helping to build the bonds that will be the foundations for a positive future. Giving children a secure and confident start in life pays dividends later for the whole of society.
- Families who enjoy secure attachments and strong bonds are more likely to weather the early years of parenting safely and build resilient children with a secure self-esteem. This will help to counteract the growing burden of mental "un-health" especially as funding for mental health services continues to decrease. Carrying (and using slings), via oxytocin release, helps to build these bonds; and can improve resilience to the Adverse Childhood Experiences that so many children experience. Read more about ACE's here.
- Anything that improves mental health and assists families struggling with PND is worth investing in, especially something as accessible and low cost as a carrier.
- A very sobering review of international attachment studies done by the Sutton Trust found that infants under three years who do not form strong bonds with a parent “are more likely to suffer from aggression, defiance and hyperactivity when they get older.” They found that up to 40% of children lack this secure bond with their parents, and this is likely to lead to their own children also suffering from insecure attachment; a vicious, repeating cycle. “Parents who are insecurely attached themselves, are living in poverty or with poor mental health find it hardest to provide sensitive parenting and bond with their babies.”
- They also found that children with weak attachment were more likely to be obese later in childhood (with subsequent effects on their long term adult health).
- Communities are the normal social structures of the human species; finding common ground and sharing the strains of life together keeps us going. Many families find community among like-minded parents; most sling users make strong supportive friendships within the sling community.
- Carrying keeps us active; movement is essential for health and fitness. Dynamic carrying in arms (if possible) helps children to hone their growing neuromotor skills, and carrying young children (or those with tired legs) is good for adults too; bone remodelling, muscle health and posture.
- As the rates of breastfeeding are higher in carried babies, the health benefits of breastfeeding will be more marked in societies who carry a lot (reduced breast cancer risk, reduced osteoporosis, increased transfer of antibodies, to name just some.)
- Babies who are carried are more content and cry less. Crying is very stressful; and successful calming of a distressed baby will build a parent’s confidence in their ability to care for their child and also reduce the feelings of tension in social gatherings or in large public open spaces.
- Carried babies may have had less ear infections, less corrective treatment for plagiocephaly, and thus have been less in need of the NHS budget.
I believe that health care professionals should therefore promote frequent carrying of infants to achieve the best possible outcomes for families, and for the long term benefit of the societies they live in. It is a low cost intervention that can have far-reaching effects.









Positive Effects of Carrying for Parents and Carers
In-arms carrying and using slings doesn’t just bring good things to babies – they can make a real difference to parents and other caregivers too. Read more about the benefits of babywearing for adults here.
- It encourages bonding and deepening of a loving relationship via the release of the hormone oxytocin; having baby close heightens the parent’s awareness and can increase their responsiveness to their baby’s needs. You can read more about the effects of oxytocin here.
- It can increase parental confidence. The parent may be more “in tune” with their baby, as the carried child is part of the parent’s personal space, and the parent will be more aware of changes in a child’s mood, and thus be more able to respond to the child’s facial expressions, gestures and vocalised needs sooner. This will build mutual trust and contentment.
- There is evidence to suggest that sling use can help with perinatal mood disorders such as postnatal depression, in part due to oxytocin release and in part due to increased bonding.
- Fathers and other care-givers will be able to use a sling as well, increasing family connections and helping baby recognise more people by their voices and scent. Sling use can be very valuable in giving family members “cuddle time” and can be an useful tool for childminders as well.
- Slings can provide “hands-free” parenting, which can be very useful, such as making a quick snack, interacting with an older child, doing the housework or other chores. A “fussy” baby may calm and settle in a sling, allowing the parent more choice about how to use their time.
- Slings can provide opportunities for physical exercise and mental stimulation; a new skill to learn and a new social circle (social sling meets, for example!) Many people find that carrying their children on walks helps to lose weight and tone muscles. Dynamic (in arms carrying) is also a good workout!
- Slings can provide greater access to the world – in a good sling the only limitations are where your feet can take you. Onto the beach, off the beaten path, up a tower, onto crowded public transport, around busy airports, the world is your oyster!
- Slings can provide comfort and nurturing for older children as well.

Positive Effects of Carrying for Baby
Carrying your baby is essential to their normal physical, psychological and neurological development. Human bodies are adapted to be a carrying species, it is part of our evolutionary history, however, our bodies are not as fit or as strong as our nomadic ancestors. It can be hard to carry in arms for prolonged periods of time. Nevertheless, babies need to be held, so a good, safe sling can be very useful in to help with increasing carrying frequency.
Remember, it is the relationship of closeness and loving touch that matters, as well as the position adopted in a good sling. The type of sling or the fabric that you use is just personal preference.
The benefits of babywearing- or the positive effects of carrying for baby are many; here are a few.
The positive effects of babywearing for baby are many; here are a few.
- It encourages bonding with the parent and helps to meets baby’s strong need for a sense of security and attachment, which will lead to greater confidence and independence later in life, as well as greater resilience and better long-term physical health.
- It helps to regulate temperature, heart and respiratory rates, and emotional and physical growth. This can be especially useful for premature babies (the term “kangaroo care” and “fourth trimester” come from this concept) or children who are unwell.
- It promotes and encourages the establishment of a successful breastfeeding relationship, in part due to the oxytocin release from the soft touch. Mothers who carry their children in soft slings are more likely to breastfeed beyond the early weeks.
- Soft touch has many benefits for neurodevelopment and and helping the social brain to form.
- Regular close skin contact is believed to help babies regulate their circadian rhythms better and distinguish the difference between night and day sleep.
 It reduces crying, both frequency and duration, (Hunziker and Barr 1986) and can improve sleep. It is safe for your baby to sleep in the sling, if the airway is well protected. Less crying means more time to be in “quiet absorption’, promoting learning and positive interactions with the world. The Esposito study discusses some of the mechanisms behind movement and how carrying is calming for babies.
It reduces crying, both frequency and duration, (Hunziker and Barr 1986) and can improve sleep. It is safe for your baby to sleep in the sling, if the airway is well protected. Less crying means more time to be in “quiet absorption’, promoting learning and positive interactions with the world. The Esposito study discusses some of the mechanisms behind movement and how carrying is calming for babies.
 It reduces crying, both frequency and duration, (
It reduces crying, both frequency and duration, (
- Babies with colic can be hard to soothe, but the motion gained from being gently rocked in a sling while the parent/carer walks may help to settle them, and also the parent/carer may feel less helpless. There is no evidence to suggest that babywearing actually reduces colic itself.
- Many parents of reflux babies spend a lot of time holding them upright and have tired arms and sore backs! A good sling that supports an upright position can thus reduce regurgitation and the discomfort of reflux. A spread squat position helps relax puborectalis muscle, to aid bowel elimination.
- The motion experienced by a baby being held by the carer allows the vestibular balance apparatus to develop more rapidly and enhances neuromotor development and muscle strength. It improves neck and head control, but is not a true substitute for “tummy-time” (tummy-time head-lifting is against gravity from a prone position). This is more marked with dynamic in-arms carrying (where this is possible). A sling or carrier should never be used as a prolonged restraint (unless danger is present such as crossing the road).
- Children should always be encouraged to be active as much as possible (WHO 2019) and if they want to get down and it is safe and practical to do so, this is ideal. However, this doesn’t mean that a child who is otherwise very active needs to be automatically removed from the sling after a certain amount of time. Sleeping babies do not need to be disturbed, just gently adjusted to ensure safety.
- It is believed to encourage sociability and language development; being able to hear the parent’s voice close up and watch their interactions with the world and other people from a higher vantage point is beneficial and also aids formation of family relationships. Studies into reduced talking in outward facing buggies highlights the importance of children being able to communicate easily with their carers.
- It allows baby to retreat from an overwhelming world and snuggle into the parent’s body for respite when needed. This is harder to do with world-facing carries, so encouraging parental responsiveness with front-facing out positions is important. (The challenges of facing forwards is covered in more depth here)
- Babies can learn very easily from a place of consistent safety, as their brains are not engaged with mere survival.
- Good, correctly designed slings that encourage the physiological spread-squat "M shape" position (that mimics hip-perching) can help prevent hip problems later in life in those children at risk of hip dysplasia. There is currently no convincing evidence that narrower based carriers cause hip dysplasia in otherwise healthy hips.
- Babies who are carried are less at risk of plagiocephaly (the flattening of the skull bones at the back of the head from prolonged periods lying on the back, more common since the “Back to Sleep” campaign). Slings are recommended as one solution (by the NHS, too!)
Further reading
"Why Babywearing Matters", Rosie Knowles, 2016
To have and to hold: Effects of physical contact on infants and their caregivers, Infant Behavior and Development, Volume 61, November 2020







Read some more articles about why carrying and using slings are good for babies below
Attachment, Babies and Carrying (HuffPost)
Secure Attachment and the Fourth Trimester
Adverse Childhood Events and building resilience in children
Seven Reasons to Carry your Baby (HuffPost)
Why Carrying Matters (Juno Magazine)
If you would like to read in more depth on this subject, my book “Why Babywearing Matters” discusses much of the evidence base for the importance of carrying. It is normal behaviour for the human species to carry their infants close to their bodies; the book considers the anthropological, physiological and psychological reasons for this. Carrying really matters.

Blog
The Carrying Matters blog page.. enjoy reading! If you have any topics you'd like to see covered, get in touch! I enjoy writing and am always keen to hear of new ideas, and to host guest blog posts too!
Can I carry my baby in a sling if I have epilepsy?
Guest Blog from a friend of mine about her choice to use a sling to keep her child close despite her diagnosis of epilepsy. It has worked out very well for her. Here she discusses the processes of…

Welcome to Slings
Welcome to the wonderful world of slings! You may be new to carrying and a bit overwhelmed about the choices available. You may be just starting out with your carrier and not sure if it’s the best or most comfortable option and wonder what else there may be. Read on for more information about how to make babywearing work for you, your baby and your family.
New to slings?
Not sure where to start when it comes to using a sling? This is a common concern among parents who have become convinced of the benefits of carrying their baby but feel a bit all at sea about the huge variety of slings and the confusing jargon in the sling community.
- There are many positive effects of using a sling with a very young baby; there is much evidence to suggest that skin to skin contact between mother and newborn (especially premature) babies can confer great advantages on both. The baby gains assistance with their physiological regulation of breathing and heart rate, temperature control is improved, and the contact helps to establish breastfeeding and promote more rapid growth compared to babies who are not held as close for as long. Furthermore, the baby will feel more secure in his developing relationship with his caregiver, due to the time spent in close contact.
- The caregiver enjoys positive effects too; he/she may find themselves more able to bond with their baby, due to the increased release of oxytocin, and post-natal depression may be reduced. Being able to be “hands-free” can really make a difference to a family’s ability to get around with their new baby, keeping them active and engaging with normal life.
- There are also many positive effects for society; such as a reduced burden of mental health and greater fitness.


Firstly, make sure you choose a sling that allows you to carry safely.
This is especially important with young babies who are still small and in need of “fourth trimester” nurturing. In summary, a baby’s airway should be supported with the head well aligned with the spine, thereby avoiding curled-up into ball positions that could impair breathing. Carriers must not be too tall, do not be tempted to tuck your baby’s head down inside a carrier for “head support”.
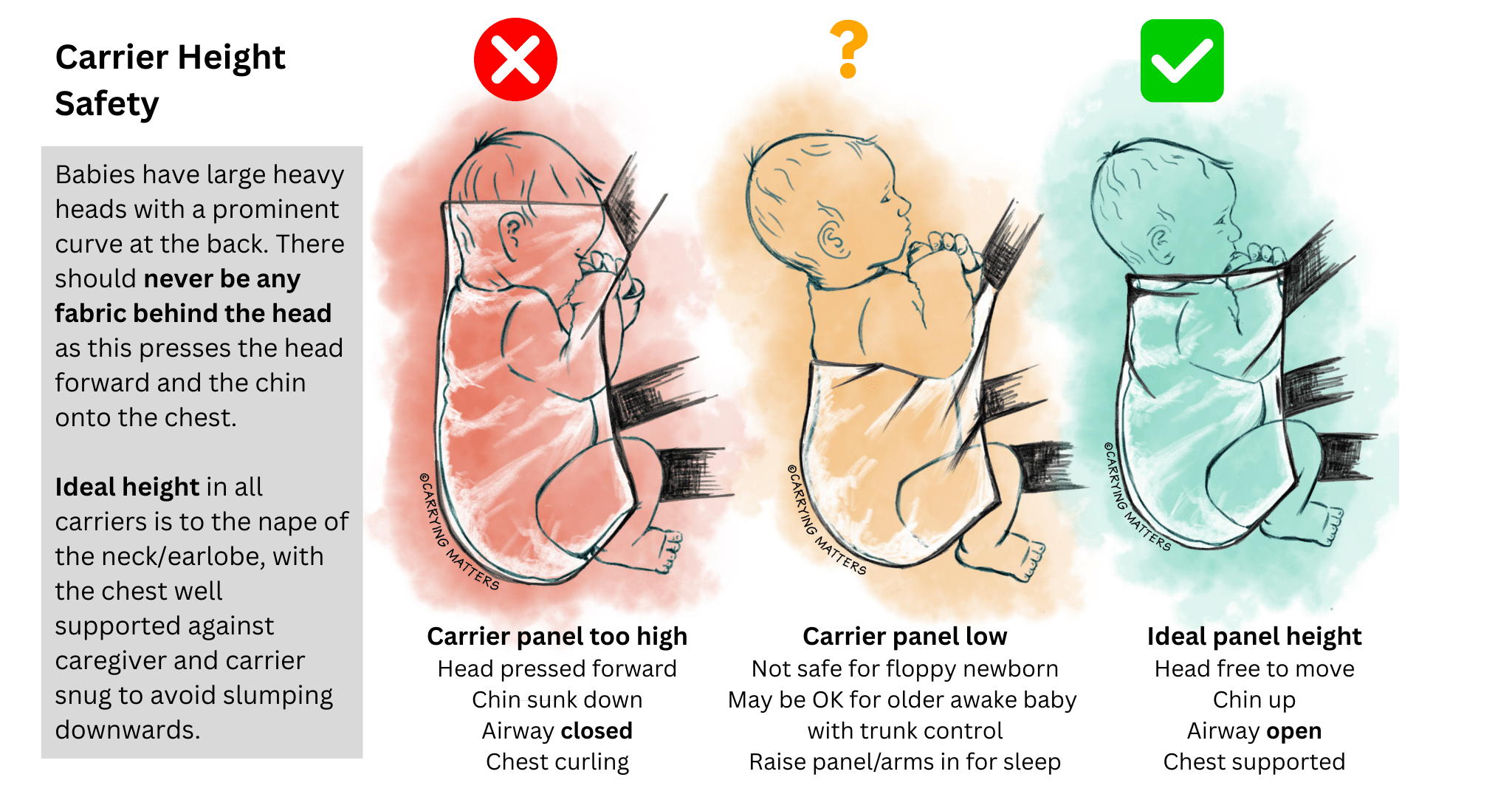 The safest place for a baby is upright, facing the parent, just as they are when carried in arms. His head should be resting against his parent’s upper chest, close enough to kiss, and supported snugly all around to avoid any slumping. Babies naturally adopt a squat position with a slightly curved lower back (you can see this in action when you lay your baby down to change their nappy).
The safest place for a baby is upright, facing the parent, just as they are when carried in arms. His head should be resting against his parent’s upper chest, close enough to kiss, and supported snugly all around to avoid any slumping. Babies naturally adopt a squat position with a slightly curved lower back (you can see this in action when you lay your baby down to change their nappy).
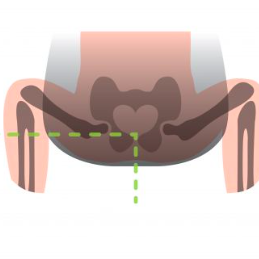
Ergonomic slings will respect this and carry a baby in a seated position, with the knees above the bottom. By bringing knees up, babies’ hips are rotated and do not need to be spread very wide to be resting comfortably, as the image shows. Narrow-based carriers (sold by high-street shops and online) are not always unsafe, but they are often suboptimal and may not be as comfortable for a baby to rest in as one that has a wider seat and encourages the knees to be raised.
Such hip-healthy positioning also helps to stabilise a baby’s back and protects the airway, as it reduces the amount of backward head lolling and uncomfortable straightening of a baby’s curved spine.
Click the link to read more about safe positioning in a sling and click here for information about healthy hip positioning.
This baby has just had her stretchy wrap removed; the sling has held her in the natural "in- arms" position

Safe, anatomically correct and comfortable positioning in arms and in a carrier

Secondly, choose a sling that is comfortable
Many parents find their high-street carriers can be less comfortable than they hoped, especially as their baby grows, and may stop using a sling at all.
Good slings have been designed to mimic in-arms comfortable carrying as much as possible, and many people find they are able to enjoy long walks with their children, up to pre-school age, with such an ergonomic carrier.
Broad weight distribution across the parent’s body matters; a child who is able to snuggle in and shift their weight closer to their parent’s centre of gravity will feel a lot lighter than one who is held in a stiff pocket, or held lower down and facing out (thus pulling away from the parent).
This applies in front, hip and back carries equally. Positioning makes a great deal of difference to your child’s and your experience of the sling, and is the most important factor in how comfortable it is.
You can make your high street carrier more comfortable in a variety of ways, for example by ensuring your baby is higher up on your chest, held snugly, and using a scarf to redistribute the weight. Your baby should be held snugly enough not to swing free when you lean forwards.
Features like the type of shoulder strap (wide or narrow, those that cross over on the back versus those that are more like rucksack straps), the shape and sturdiness of the waistband, and the type of fabric used can also make a considerable difference. It is always worth trying before you buy, and there are many sling libraries around the country that can help you do this. The Sling Pages has a full list for you to check your local resources.
"Scarf hack" for narrow based carriers

Thirdly, think about what kind of sling may suit you and your family best

Stretchy Wrap
If you have a newborn or a baby under six months, most people will start with a stretchy wrap. This is usually a long piece of jersey style elastic fabric that is between 4 and 5 metres long, and can be wrapped around your body to create a snug pocket your baby can nestle into. Depending on the quality of the fabric, the stretchy wrap is usually used up to six months. It is often worth investing a little more for higher quality.
One size (usually) fits all, and it can be tied on and left on all day for convenience, popping baby in and out with ease without needing to take the sling off each time, many parents don’t realise this. It is possible to use the stretchy wrap as a breastfeeding aid, with care and attention to baby’s airway.
You can read more about stretchy wraps here, including how to use it well.
Close Caboo Carrier
This is a slightly more structured and less stretchy variant of a stretchy wrap, with a little less flexibility. It is put on, adjusted carefully, and then baby is popped into each of the cross passes on the front. The fabric can be tightened through the rings to achieve a snug fit. The Close Carrier can be used as a breastfeeding aid if required, with care and attention to baby’s airway, and most people will find it supportive up to three to four months.
Ring Slings
This is a piece of woven fabric which has one end sewn securely into two strong rings. They are worn cuppring one shoulder with the child sitting in a pouch on the opposite side of the parent’s body, with the loose end of the fabric threaded through the rings in such a way that the tension holds the fabric firmly and the weight is distributed across the shoulder and back.
They have the advantage of being lightweight and (once the knack is gained), quick to put on and take off. They can be very useful for those who need to be able to carry their child on the hip, or need something that offers the child a good viewpoint in all directions.
Ring slings made of woven fabric and with no padded rails are usually the best option, and shoulder style (pleated or gathered) is a very personal choice. They can be used from birth to toddlerhood, and it can be easy to breastfeed in a ring sling, with the appropriate attention paid to airway and positioning.
Hip carriers
Pouches are another kind of hip carrier which can be very simple, but need to be fitted to size; they can be a risk for babies under 3months if used badly.
The Scootababy is a buckled hip carrier with a waistband which can be used from approximately four months and up into toddlerhood.
Carrying aids and hip seats can make hip carrying easier but are not hands-free.
You can read more about ring slings and hip carriers here and your local sling library will be able to help too.


Woven Wraps
Woven wraps are excellent choices if you want great comfort and longevity. They can be used from birth to toddlerhood and beyond. Woven wraps are long parallelogram shaped pieces of fabric, anything from 2 to 7m long.
They are woven in a particular way to provide gentle all-around pressure, supportive but still soft and mouldable. Most woven wraps are made of cotton, some may contain other fibres such as linen or hemp, for extra support, and come in many different colours and designs.
Many women around the world use local woven cloths for many purposes as well as for child-carrying. These cloths and woven wraps feel very different from the fabrics you might find in a haberdashery shop; these are more likely to fray and tear.
Many people begin with a 4.6m wrap (known as a size 6) and learn a carry known as the Front Wrap Cross Carry. They can take a little practice but they allow a great degree of adjustability and weight distribution around the body. There are numerous ways to tie the same wrap, so they can be used on the front, hip or back at the appropriate ages. Your local sling and carrier consultant or sling library will be able to get you started!
Upright breastfeeding is possible, if done safely with the appropriate attention paid to airway protection.
You can read more about woven wraps here.




Meh Dai/Bei Dai (formerly known as Mei Tai) Carriers and variants (half buckles, onbuhimos, etc)
These are Asian inspired carriers made of soft fabric, and are popular with those who appreciate the mouldability and support of woven wraps but need something with more structure, or speed of use.
They consist of a fabric panel that has two straps at the base which are tied or buckled securely around the waist, and two straps from the top of the panel which can be wrapped around the parent and baby to ensure a snug and comfortable fit. Baby sits in the pouch created by the panel, and the long straps allow a great degree of adjustability to all shapes and sizes. They can be worn on the front, hip and back at the appropriate ages, and upright breastfeeding is often possible, if done safely with the relevant attention paid to airway protection.
Your local sling library should have a few of these to try out.
You can read more about meh dais and their variants here.
Full Buckle Carriers
If you’re not sure about tying fabric, a good option is a full buckle carrier, which has a buckle on the waistband, and the shoulder straps buckle into the panel at the sides. Baby is seated facing the parent, inside a supportive pouch that supports them widely across the base from one knee to the other.
Waistband types vary, from the minimal to the heavily padded, and people’s preferences vary enormously. Some shoulder straps cross over on the back when baby is on the front, others are fixed into a rucksack style. The shape of adult and baby together is very individual, as is the health of the adult’s back, so what suits one pairing will not suit another. More padding does not automatically mean “better” or more comfortable, and those with back pain will not always need heavily structured slings. Good posture and general back health are important – read more about this here.
Buckle carriers can be very quick and simple to use. Often, a little practice to get the straps and positioning optimally adjusted is well worth it. Most good full buckles fit well from three months upwards; some can be adapted for younger babies by rolling the panel or by using inserts to keep baby snug, high up and visible. Many carriers will last into early toddlerhood, and some beyond that, depending on design.
Many mums find that breastfeeding in the buckle carrier is possible, if done safely with the relevant attention paid to airway protection. Most can be used on the back once babies have grown.
Some buckle carriers will allow baby to face the world. This can be great, when done safely and responsively. It is recommended only from four months upwards, not for sleeping in to protect the airway, and only for short periods of time. This is due to the reduced opportunity baby has to see and interact with his parent and learn about the world based on his parent’s response to it – this is known as social referencing. There is also reduced hip and leg support from the narrow base which can be an issue in some circumstances, as well as less comfortable for child and parent. Carriers that provide hip healthy positions facing out are generally preferred. (read more about facing out here.)
You can read more about buckle carriers here.




Fifthly, enjoy your sling and let the world see it!
Why not share your enjoyment with the parents you meet so they can discover slings too? We all carry our babies, some in arms, some in high street carriers, some in wraps, some in ring slings, some in meh dais, some in buckles. We all learn from each other; encouragement is always more productive than criticism!
Here is a lovely article from Ellie at Peekaboo Slings about the importance of no judgment; “We want to normalise babywearing and promote carrying your children close – put bluntly, we don’t care about the rest”.
Fourthly, be aware of the changing needs of your baby
The weather conditions may change how you carry your baby; being aware of the heat and the sun, or the cold and the rain may affect your choice of sling and your clothing.
As your baby grows, her own needs will change. She may want to sleep less and look around more. She may prefer hip carries, or even back carries, so she can see into the world into which she is being carried. As she gets heavier, the carrier you began with may begin to feel less supportive for you and for her; for many this marks a move towards “toddler-worthy” carriers. This may be different ways of tying your woven wrap, learning how to adjust the straps on your meh dai to ensure knee to knee support, or moving up to a bigger, toddler-sized (or even preschooler!) carrier when you need to. Your “baby” sized carrier will often last a lot longer than you think.
You will not spoil your baby or make him clingy by carrying him as he grows. Big kids need cuddles too – loving contact is vital to our emotional health and security, from cradle to grave. You can read more about carrying older children here, and your local sling library or consultant should be able to help you make the most of your carrier.

Carrying in the Postnatal Period

Is carrying in the postnatal period (in the early weeks after a baby is born) safe?
Babies want to be held close from the very moment they enter the outside world; they crave contact and many will spend their first few days and weeks sleeping in their parents’ arms and feeding frequently, enjoying this close interaction.
Pregnancy can be tiring and uncomfortable for many, due to our changing bodies and habits. We are no longer an upright species but a sedentary one, to our great anatomical and physiological disadvantages; chronic pain is a significant problem for increasing numbers of people in our society. Symphysis Pubis Dysfunction can be debilitating for pregnant women, and there is a growing belief that many women’s bodies are frequently not in the optimal condition to carry a child and thus take much longer to recover from pregnancy than our forebears. Ligament softening and laxity (from the hormonal changes preparing a body to deliver a fetus) can take some time to resolve fully especially if there has been pre-existing back pain and poor posture, and breastfeeding may prolong the effects of relaxin.
Labour, while exhilarating and empowering for some, can be exhausting for others, especially if prolonged. The recent historical practice of lying down for delivery is in marked contrast to how most women around the world across history and cultures have given birth (upright, squatting or kneeling). The natural birth movement and the emergence of doulas to support women with their delivery choices mirrors a growing desire to get back to our ancient human roots, which may also encourage speedier recovery from labour and birth.
 Women are becoming prouder of their bodies and what they have achieved; bringing forth life. As a friend of mine once said, how can you ask a butterfly to return to being a caterpilllar? Women's bodies are designed to carry and nurture children before birth and after. Here is a photo of one mum carrying her newborn in the early days after birth, proudly showing her post-partum body.
Women are becoming prouder of their bodies and what they have achieved; bringing forth life. As a friend of mine once said, how can you ask a butterfly to return to being a caterpilllar? Women's bodies are designed to carry and nurture children before birth and after. Here is a photo of one mum carrying her newborn in the early days after birth, proudly showing her post-partum body. 
The rate of caesarean sections (both planned and as emergency) is high in Western society, currently between 20-25% of births in the UK (with some regional variation). A caesarean section is major abdominal surgery and some recovery time from this is to be expected, and varies enormously from woman to woman, depending on the reasons for the operation. Women are advised to avoid heavy lifting, “carry nothing heavier than your baby”, and not to drive for at least six weeks after birth. Scars can be uncomfortable and slow to heal for some, and some may experience abdominal pain for a while afterwards. Babies may come early and be very frail for several weeks.
Therefore it is not surprising that many mothers worry that after labour and birth, they may not be strong or well enough to carry their newborns in their arms for prolonged periods. Many will have toddlers at home needing the reassurance of their mother’s loving arms to help them cope with the newcomer’s arrival. Paternity or parental leave is often short; in a few weeks mothers are often required to manage at home alone.
Carrying your child in the postnatal period is important.
The early weeks are vital for bonding and attachment, providing continuity and security, promoting breastfeeding and helping to reduce depression. So yes, we should carry our babies somehow after birth. This doesn’t need a sling; people can hold their babies while sitting down and while reclining just as much as while they stand and walk around; it is the closeness and the contact and the skin to skin that promotes bonding and oxytocin release that matters. It helps to shape baby's brain, and also has a positive effect on yours! Furthermore it can be a great way to ensure any older children still feel connected to you, as your hands are free.


Carrying a newborn baby can be very healing if birth has been traumatic or there has been previous bereavement.
“"I had a tiny baby (4lb5oz) and experienced a traumatic birth, I suffered with PTSD. At times this meant I was very anxious and wanted to keep my baby close to me to be sure she was safe. I started with a stretchy wrap when P was just 3 weeks old. I truly believe babywearing strengthened my attachment with her and helped me to cope every day." Anon
There are some garments of clothing that can be worn in hospital or in the early weeks after birth; mimicking the practice of putting a tiny newborn down the front of the shirt. Some of these garments (known as skin to skin tops or kangaroo care clothing) are designed for keeping baby skin to skin to the parent while reclining, and are not hands-free.

Others are a little more structured (at least two layers of stretchy fabric) and provide enough support for baby that a parent can be hands-free and walk around, similar to a stretchy wrap. These can be most useful in hospital environments for their coolness and simplicity.
Please note that if your baby is premature or very small (under 6lb) it is wise to seek the advice of a specialist baby-carrying consultant; many "newborn" carriers, including some stretchy wraps will not provide enough support without guidance on how to use for these babies with special needs, and many buckle carriers will be much too big.
Breast and bottle-feeding can cause back, neck and shoulder pains, as can prolonged periods of one-sided carrying (which can also affect the pelvic floor and the symphysis pubis.) Being alert to the body’s signals of discomfort and acting on them to frequently redistribute the strain is of great benefit in building up tolerance and strength.
As women recover their strength and are able to do more each day, their mobile carrying abilities will grow too. As womens’ bodies settle back down after pregnancy, with appropriate pelvic floor toning and correction of posture and alignment, carrying will become easier. Furthermore, as baby gets bigger and heavier, the parent’s muscles will adapt to the gradually increasing weight and become more toned day by day, the more often they carry.
“Much of my pre-pregnancy life was spent in the mountains, and carrying my babies after their birth helped me get back in touch with my "home". It enabled me to very gradually and gently regain some fitness away from busy streets, and felt like less strain on the scar area than pushing a double buggy uphill.” Carissa

Keeping a baby’s weight high, snug and central will encourage loading across the large weight-bearing axes of the body, thereby preventing strain on muscles, ligaments and the pelvic floor, and avoiding abdominal pressure. Lifting a baby to the chest should be done carefully, with knees bent and upright posture maintained, and pelvic floor and core muscles engaged and active. Most types of carriers will be possible to use after a vaginal birth, and it will be a very individual and personal choice which. On the whole, most babies enjoy the gentle all-around pressure of carriers that can mould softly around them and be reminiscent of the uterine walls they have just left; and carriers that distribute weight widely across the parent’s upper body will be more comfortable.
If you have a sling that makes your back ache, please visit your local sling library or consultant for a fit check (often a few tweaks make all the difference) or to try an alternative. Cheaper carriers from supermarkets/Ebay often work much less well than better designed carriers and therefore last much longer. "My baby is too heavy for a sling" is usually an issue with the sling not fitting/not being well designed.
Carrying after a Caesarean


This is also very possible, and it could be argued, perhaps more important post section than after a normal non-instrumental vaginal delivery, depending on how the individual feels after the surgery. Achieving skin to skin as soon as possible is ideal, for promoting oxytocin release and bonding. This is vitally important after a section, especially if it was emergency and traumatic, thereby interrupting many of the biofeedback mechanisms around bonding. It is also important if the section was planned and baby was thus delivered before the biological hormone cascades of labour and birth were able to begin. There can be a strong tendency for women who did not have the birth experience they wished for to feel robbed and deprived of an important part of their baby’s arrival. The subsequent feelings of sadness and grief, or disappointment or that they have let themselves or their baby down somehow, however untrue, can significantly hamper the forming of attachment bonds and play a part in later postnatal depression or other mood disorders.
Mothers who experience this are very likely to find that skin to skin contact and frequent close touch and carrying extremely useful; the process of initiating and mantaining contact and loving touch often acts as a catalyst for the oxytocin release; this positive feedback mechanism will encourage loving feelings to develop despite the less than “perfect” start and get bonding well under way.
As soon as surgery is safely over and a well baby can be given to its mother, skin to skin can begin; resting on the mother’s chest under a blanket, inside a shirt or with kangaroo care clothing. Women are entitled to this skin to skin and should insist upon it; baby does not need to be washed or the cord to be cut before contact is achieved; the sooner the better.
Once mother is ready to move around and carry her child in her arms she can; she is advised to carry nothing heavier than her baby. Some women will choose to use slings immediately, if they feel ready (especially if they are already familiar with slings and feel confident with their use), others will wish to wait, especially if they feel unwell or are in pain. If the mother is confined to hospital and alone for parts of the day and wishes to move around, she may find the sling will help her to feel safer than carrying her baby loose in arms while she is still a little unsteady.
“Having a sling for carrying was very useful, as much easier and less painful than carrying in arms (less stress on abdominal muscles). It was great for bonding, especially since we were having trouble with breastfeeding.” Rebecca
The key factor is to avoid any carrier from irritating the wound or putting pressure on the abdomen. Double layer kangaroo-care shirts or other soft carriers such as stretchy or woven wraps, high-carrying waistband-less meh dais or buckle-tais and ring slings in frontal tummy to tummy carries, may be options to consider. Baby’s legs should ideally be tucked into the M shape, and this will also help to avoid feet kicking against a still tender wound. As the scar and any abdominal pain heals, carriers with more structured waistbands will become more accessible.
General tips about post-partum carrying (including fitness classes)

 Baby carrying in the post-partum period is possible, if done in a mindful, responsive way, and can actually help promote recovery. Holding a baby close in the anatomically correct position so that their weight is well distributed through the large weightbearing axes will tone muscles and improve posture more than pushing a pram with a strong forwards lean. Being able to go for gradually longer and longer walks with your baby in a soft and comfortable sling will rebuild strength and release endorphins which are natural feel-good hormones.
Baby carrying in the post-partum period is possible, if done in a mindful, responsive way, and can actually help promote recovery. Holding a baby close in the anatomically correct position so that their weight is well distributed through the large weightbearing axes will tone muscles and improve posture more than pushing a pram with a strong forwards lean. Being able to go for gradually longer and longer walks with your baby in a soft and comfortable sling will rebuild strength and release endorphins which are natural feel-good hormones.
Participating in postnatal recovery programmes can be useful; however combining carrying and exercise/dance is usually best done with great caution as not every provider will have adequate knowledge about postnatal recovery (pelvic floor and diastasis recti issues) or about the rate and speed of each woman’s individual recovery from birth. Many may have no specialist knowledge about safe sling use or how to protect a baby from sudden shaking movements, as well as how to avoid overloading still-recovering tissues with certain stretching or weight-bearing activities with the extra load of a child in a sling. Walking with a baby in the sling, ensuring good alignment and posture, gradually increasing the speed and duration, is usually enough exercise for most women in the early months. Please do not rush; pelvic floor dysfunction is very very common (14 million women in the UK are known to have an issue, and many many more never seek help and remain undiagnosed). Leaking is NOT normal or to be expected. If you are unsure if your pelvic floor is recovering normally, please see your GP.
Read more about babywearing fitness classes here.
Using a sling allows families to settle back into the normal rhythms of daily life.
Often, older siblings are uncertain about the new addition to the family and uneasy about their place in it; they may need extra reassurance with the birth of a new baby. They may wish to return to their mother’s arms and be close to her body, for reassurance and reinforcing of the attachment bond.
Toddler carrying after birth
“During the intense post-birth bonding period with D I began to use a couple of wraps that had been favourites of R (the new big brother). It almost felt like a betrayal! But one afternoon, R asked if he could come up for a front carry in his favourite wrap, something he hadn't done for ages, and we twirled round the lounge together laughing while my husband cuddled the new baby. I think that was a really healing moment for us and let my eldest know he still had an important place in my arms too.’ Emma
However, toddler carrying after birth is much more of a challenge, especially if the pelvic floor is weak and there is diastasis recti (separation of the abdominal muscles from the stretching during pregnancy). Please seek help if your floor or core are weak.
 Many specialists would suggest it is wise to wait until any pelvic floor/diastasis recti issues have resolved and the mother is functionally strong before beginning to carry toddlers again; this will of course vary widely from woman to woman. Generally those mothers who are well used to carrying toddlers will find it easier to resume carrying than those beginning for the first time, and front carrying may be the most suitable position (rather than hip or back carries, to avoid straining still-healing tissue). Sitting down cuddles may be wise for a while!
Many specialists would suggest it is wise to wait until any pelvic floor/diastasis recti issues have resolved and the mother is functionally strong before beginning to carry toddlers again; this will of course vary widely from woman to woman. Generally those mothers who are well used to carrying toddlers will find it easier to resume carrying than those beginning for the first time, and front carrying may be the most suitable position (rather than hip or back carries, to avoid straining still-healing tissue). Sitting down cuddles may be wise for a while!
Involving the whole family!
The post-partum period may be a great opportunity for other caregivers in the family to share the carrying and begin the bonding process. Whole families thrive when children are kept close; it spreads the load of child care around. Partners can carry their newborns, or their older children to provide reassurance.
“Carrying our eldest son (3) enabled my wife to give her attention to our new baby. It gave us much needed daddy and son bonding, at a time when he was feeling insecure with the arrival of the new baby.” Mal
Remember, it is the closeness and contact that matters; in arms carrying is as valuable as using a sling, and the shifting of your growing baby around your body as your muscles tire will help to rebuild your strength and endurance. Sharing the carrying with other members of your family will help to strengthen relationships and reduce the strain on your own body too.


Carry Me Daddy!
“Dear Daddy

When you hold me I feel happy. You are strong and I am safe in your arms. The more time I spend with you the more I trust you, and the more I can let you look after me when Mummy isn’t here.

I love to hear your breathing and the sound of your voice rolling around in your chest. I can hear your heart beating and it steadies me. I can hear you best when I am close to you. I love it when you look at me with your proud eyes, it makes me feel good. I feel loved.
I love being carried on your chest where we can chat till I am ready to snuggle contentedly to sleep.
I love my rides on your shoulders and on your back. The world is so interesting from up high!
I love the games we play and the way you make me laugh till I have no more breath in my body. I love it when you hold me on your lap to read to me. I love it when you hold my hand.
Carry me Daddy, while you still can!”












In-arms carrying and all other means of close and regular contact (such as noisy physical play) is of enormous value in building bonds between fathers and their children. 1 in 4 children lack strong attachment relationships, and slowly our society is recognising the need to address this. In arms carrying can be hard work, and a good comfortable baby or child carrier can make this much easier. Babywearing dads are becoming more and more visible, which is great news for families and for our society.
There can be a common myth that is only mothers who bond with their children in depth, and that the changes in her brain with parenthood are unique to her. This isn’t the case, fathers’ brains are also deeply affected by their caring role and they form strong, lifelong connections to their children if they are closely involved with their young baby as they grow. Bonding can be encouraged in many ways, not just though feeding the baby (which is another common myth). Babywearing is one tool for developing a deep relationship.
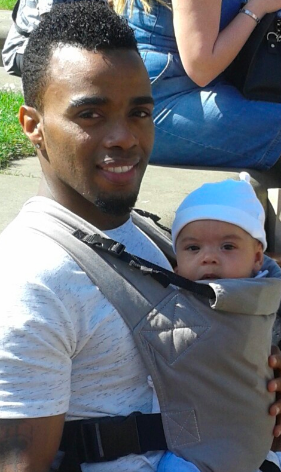
Here are some fathers talking about babywearing, what it means to them and why they do it!

Mohamed
Babywearing! How are you faring? Are they still staring? As a father of twins who liked getting things done, there was only so far my two hands could take me when I had two babies to hold. I was hesitant at the science behind stretchy slings when I was first told you could carry more than 1 baby in them, the picture shows how quickly that evaporated into pure elation and joy. "I've got my hands back!" I remember thinking. That was the start to an awesome journey where there was nowhere I couldn't go with the twins. Beyond the physical strength which babywearing gave, I feel like it helped me show my girls that no matter what, I was able to lift them and raise them above whatever it was they were facing and give them a different view while still supporting myself. Why are you fearing if all you are doing is baby wearing?

Perinatal Mood Disorders and Carrying
The prevalence of Perinatal Mood Disorders (pre and post-natal depression, anxiety and post-traumatic stress disorder) is increasing in Western society as it is increasingly fractured and isolated, with a decreased sense of local community and shared care. The birth of a baby is often an overwhelming time for both parents, especially when also faced with the expectations and demands of a fast-paced culture that often judges people by their apparent productivity and appearance. As a GP, I see many families struggling with these conditions that are often diagnosed, and keeping babies close may play a part in surviving these illness, mainly due to the closeness with your child, rather than the choice of sling.
Postnatal depression is on the rise – affecting at least 10-15% of new mothers (with many more sufferers (and fathers) never being recognised to have the condition). Anxiety and PTSD are also worryingly common. Parents are encouraged to put their babies down as much as possible and regain their old lives; babies are expected to learn independence as quickly as possible and stop relying on their parents for their every need.
This approach to caring for children is very new in human history and runs counter to attachment theory, which suggests that the human infant thrives on responsive parenting and close contact.
Read about Ruth’s experience of antenatal depression here; for the rest of this post we will focus mainly on postnatal depression (PND).
What is Postnatal Depression?
Postnatal Depression is a depressive illness which affects between 10 to 15% of new mothers. Many more are never diagnosed with this condition, which can become a very significant issue in the functioning of a family. It is often poorly managed by health care providers, and can be misunderstood by the community and dismissed as “just the baby blues” or “tiredness.” It is common for sufferers to feel very alone and unable to explain just how they feel and why it is so difficult to endure. Prenatal depression is also experienced by many new parents, and postnatal anxiety and Post Traumatic Stress Disorder are also commonly experienced pre and postnatally.

Why is it so common?
Western society is increasingly fractured and isolated, with a decreased sense of local community and shared care. Depression is common in our culture, for reasons not clearly understood, but partly due to the way we live. The birth of a baby is often an overwhelming time for both parents, especially when also faced with the expectations and demands of a fast-paced culture that often judges people by their apparent productivity and appearance.
Before parenthood, people’s identities are often based on their roles and responsibilities in life; work, friendship circles, hobbies and interests. After a baby arrives, this often changes dramatically, sometimes in unexpected ways, and for many, the huge change in the pace of life and the loss of control can be very difficult to deal with. “The burden of conscious responsibility with no let up and the unusual and unexpected degree of fatigue can make a mother feel desperate about whether she can survive and how she will manage.” (Kennell & Klaus) This is the role that community used to play; supporting and carrying each other’s burdens as part of a committed and close-knit group of people who lived together, an experience that few parents enjoy in the West today.
What does it feel like?
Common words used to describe PND are guilt and inadequacy.
“The worst part was the guilt I felt about crying every day when I had a beautiful new daughter.”
“It isn’t about not loving your baby but about feeling overwhelmed with responsibility and unable to cope.”
“My head can feel empty and I have no thoughts.”
“It is just so hard to face another day of feeling totally unlike myself, missing my old life, unable to enjoy this new one.”
Fathers suffer from depression after birth too.
“The first few weeks were the hardest and I would just sit and cry. I felt like this shouldn’t happen to me, I should just be taking it on the chin and getting on with it. But the truth is, I felt alone and without the support of my wife, I would’ve been a lot worse.”
Many parents with PND feel a sense of dissociation and detachment from the child they want to love so much.
“It isn’t about not loving your baby but about feeling overwhelmed with responsibility and unable to cope.”
Caring for people with PND is hard.
“PND is the scariest and loneliest place on the planet and puts a terrible strain on the whole family.”
“My husband felt helpless because he knew something was wrong but I wouldn’t admit it and shut him out. All he could do was try to look after me and be there when I finally admitted it. It caused a lot of irrational arguments.”

What can I do?
If you are suffering, or think you may be suffering from perinatal mood disorders, first be reassured that you are not alone and the vast majority of people with it survive with few long-term ill effects.
Here are some suggestions that may help.
Get help where you are.
Tell your nearest and dearest how you really feel.
“I found the hardest bit was to admit that I wasn’t coping, even when it looked like I was, I was fine on the outside but was a complete mess on the inside.”
Many women testify how supportive their partners and families and close friends are once they understand – ask them to help with the basic jobs of daily life; cooking, cleaning etc. Help them to see how useful you will find it when they listen to you with acceptance and without judgement, and how their understanding when things go wrong is vital. Guilt is a large part of PND and many kind people may inadvertently add to this burden.
Get help from your local health care providers.
This may be your GP, your midwife, your health visitor, your local SureStart centre. The quality of care from these resources can vary enormously. It can help to write down on paper how you feel in advance and what you think you need (validation, formal counselling, CBT or medication, for example) and take it with you to appointments. Continuity of care is great, if available; a HCP who listens and cares can make a greater difference than one who fires questions and is keen to tick boxes and prescribe medication at once.
“Guilt and lack of confidence are so typical of PND and my HCP was essentially validating those feelings even though objectively I was doing a great job!”
Be armed with information (e.g. if you wish to carry breastfeeding, sertraline is safe in these circumstances). The Breastfeeding Network is a valuable resource. If you are not satisfied with the care you are receiving, find different care.
Get help from your local non-NHS resources.
These can be very useful, such as HomeStart (a befriending service) and local PND groups. A postnatal doula may help, and there are many national helplines and resources (see below)
Get help from online social resources.
There are many forums and parenting groups full of people who know how you feel, and will listen and share. Being among people with the same values and parenting beliefs may be a source of great encouragement. Equally, avoid too much time online.
Get out!
It can be very hard to actually get out of the house when struggling with dark thoughts or hopelessness, but it is worth the effort involved. Even a walk down the road is a good start, and encourages release of endorphins (the natural feel-good hormone). Arrange to meet some friends, and ask them to encourage you to come. Try to make a plan for most days, and be kind to yourself if you decide on a pyjama day instead. Try to arrange some time to spend alone with your other half, to remember who you still are, as well as parents.
Get nourishment.
Good quality food, drink, exercise and sleep are vital to your own health and sanity, as are times to enjoy the things you used to. Dress well in bright mood-enhancing colours. You are still a person and your own needs should be met as much as your child’s. Some people make use of night-time carers to allow some much-needed uninterrupted sleep.
Get past your birth story.
For many women, recovering from birth takes a while, especially if it was not the hoped-for experience. The NHS Afterthoughts service and counselling can help if you feel a sense of grief.
Get a sling or carrier.
Keeping your baby physically close is well known to stimulate the release of oxytocin. Oxytocin is a hormone that is closely related to bonding and attachment. It is released during labour and breastfeeding, and, crucially, during skin-to-skin contact and social interaction. It has an important role in encouraging nurturing feelings and a sense of belonging, and reduces anxiety and depression by affecting cortisol release.
Babies who are in close contact with their parents have been shown to have a corresponding higher level of oxytocin than their non-carried counterparts; which subsequently helps to reduce baby’s own stress levels and improve their sense of secure attachment; their needs are met at the point of request. Calmer babies are easier to care for; win/win.
The soft touch of close skin to skin contact reduces the release of cortisol, the stress hormone, via C afferet fibres affecting receptors in the hypothalamic-pituitary-axis. Stroking has been shown to reduce pain responses.
Modern life is fast-paced and for many, constant carrying of ever-growing children can be difficult to achieve, or uncomfortable after the travails of birth. This is where the practice of using a sling, (sometimes known as babywearing) can be of great value. A soft sling that allows you to keep your child close to you, (thereby stimulating the release of oxytocin and reducing cortisol), and helps your baby to relax and sleep in secure comfort may make a huge difference to your life and your feelings and help you to feel that you can cope. Anxiety may settle a little as you know your little one is safe next to you.
“The sling brought us back to an almost pregnant-like state, with him a part of me, listening to one another’s cues. He was calmer for being close to me, which made me feel more confident, which brightened my mood. Leaving the house felt less daunting so I got more exercise and again increased my confidence. I talked to him more, whether he was awake or not, and he became my son rather than a tiny scary stranger.”
“My favourite thing in the whole world, that never fails to calm me or lift my mood has been cuddles with my baby, particularly skin-to-skin. For me, there is no antidepressant like it.”
“When she was in her pram I felt completely removed from her and her world. I was just an accessory, she was a job to do and I was irrelevant. Using a sling finally helped me bond properly with her and made a massive difference to the PND.”
Many slings are extremely comfortable to use, and can be very practical indeed. It is possible to learn how to feed discreetly in a sling, allowing you more flexibility about being out of the house for the day with your baby.
Slings give you and your baby the freedom to be on the move together, rather than feeling stuck; to go out into the world for a walk or go shopping without struggling with the complexities of a pram. Movement and exercise are vital to wellbeing; and using a sling safely can help your body recover from birth and become stronger.
Slings can be beautiful and colour therapy can help to lift the mood. Learning a new skill can be therapeutic, and many parents find a great sense of community among other sling users both locally and online. This can help with feelings of isolation, especially if you have chosen to parent differently from your family or your peers.



Get a sense of perspective.
What matters in these early months is you and your baby. It does not matter what other people think; the house does not need to be pristine, you do not need to impress people with how well you are taking to parenthood. I have heard many women describe how they “are falling apart on the inside”.
“I thought because I wasn’t suicidal or not looking after things that it couldn’t be PND so held back for a long time from accepting it and getting help.”
“I found the hardest bit was to admit that I wasn’t coping, even when it looked like I was, I looked fine on the outside but was a complete mess on the inside.”
Get confident again.
Reflect on what you have achieved so far and use that to build self-belief. Learn to trust yourself, be an instinctive parent – and you will fin that as you encourage others, you will find yourself lifted too. Some people find going back to work can be very helpful; the chance to use skills again and have adult interactions once more can be a great boost to self-confidence.
Useful Resources
Postnatal Depression Information Leaflet
Postnatal Depression Information Leaflet 2
Pre and Postnatal Depression Advice and Support (PANDAS)
Mothers for Mothers Postnatal Depression Support
Postnatal Illness Information (PNI)
The Impact of Babywearing on Mothers’ Mental Health – Aimee Gourlay
Further Reading
“I carry my heart in a sling” – a blog on how slings helped Lindsay fight her PND.
Sling Sally’s talk on Slings and Sanity for the 2015 Northern Sling Exhibition
Surviving PostNatal Depression – Selina Shaik for MIND
How Carrying Helped My Recovery – Ellie at Peekaboo Slings
Carrying With A Mental Health Disorder – Andrea’s story